
Imitrex
Dana Stearns, M.D.
- Instructor in Medicine
- Harvard Medical School
- Massachusetts General Hospital
- Boston, MA
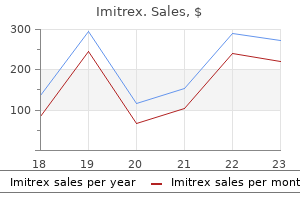
Fluids may be administered if the patient is dehydrated spasms treatment buy 25 mg imitrex otc, and antibiotic agents may be prescribed if the patient has an underlying respiratory infection muscle relaxant quiz generic imitrex 100 mg buy on line. If the patient requires intubation because of acute respiratory failure quercetin muscle relaxant purchase 100 mg imitrex free shipping, the nurse assists with the intubation procedure muscle relaxant definition generic imitrex 25 mg online, continues close monitoring of the patient, and keeps the patient and family informed about procedures. A major challenge is to implement basic asthma management principles at the community level (Reinke, 2000). Key issues include education of health care providers, establishment of programs for asthma education (for patients and providers), use of outpatient follow-up care for patients, and a focus on chronic management versus acute episodic care. Methylxanthines (theophylline [Slo-bid, Theo-24, Theo-Dur]) are mild to moderate bronchodilators usually used in addition to inhaled corticosteroids, mainly for relief of nighttime asthma symptoms. Leukotriene modifiers (inhibitors) or antileukotrienes are a new class of medications. Leukotrienes are potent bronchoconstrictors that also dilate blood vessels and alter permeability. Leukotriene inhibitors act by either interfering with leukotriene synthesis or blocking the receptors where leukotrienes exert their action (Boushey, Fick, Lazarus & Martin, 2000). At this time, they may provide an alternative to inhaled corticosteroids for mild persistent asthma or may be added to a regimen of inhaled corticosteroids in more severe asthma to attain further control. In addition, combination products are also available (eg, albuterol/ipratropium [Combivent]) and offer ease of use for the patient. Short-acting beta-adrenergic agonists are the medications of choice for relieving acute symptoms and preventing exercise-induced asthma. From Facts about controlling asthma, National Asthma Education and Prevention Program, National Heart, Lung, and Blood Institute. Volume is measured in color-coded zones (right): the green zone signifies 80% to 100% of personal best; yellow, 60% to 80%; and red, less than 60%. If peak flow falls below the red zone, the patient should take the appropriate actions prescribed by his or her health care provider. Patient teaching is a critical component of care for the patient with asthma (Plaut, 2001). Multiple inhalers, different types of inhalers, antiallergy therapy, antireflux medications, and avoidance measures are all integral for long-term control. This complex therapy requires a patientprovider partnership to determine the desired outcomes and to formulate a plan to achieve those outcomes. The patient then carries out daily therapy as part of self-care management, with input and guidance by the health care provider. Patient Caregiver Chapter 24 Management of Patients With Chronic Obstructive Pulmonary Disease 595 Lung and Blood Institute. The nurse emphasizes adherence to the prescribed therapy, preventive measures, and the need to keep follow-up appointments with the primary health care provider. A home visit to assess the home environment for allergens may be indicated for the patient with recurrent exacerbations. In addition, the nurse reminds the patient and family about the importance of health promotion strategies and recommended health screening. Other criteria indicating the need for hospitalization include poor pulmonary function test results and deteriorating blood gas levels (respiratory acidosis), which may indicate that the patient is tiring and will require mechanical ventilation. Although most patients do not need mechanical ventilation, it is used for patients in respiratory failure, for those who tire and are too fatigued by the attempt to breathe, or for those whose conditions do not respond to initial treatment. Infection, anxiety, nebulizer abuse, dehydration, increased adrenergic blockage, and nonspecific irritants may contribute to these episodes. A ventilationperfusion abnormality results in hypoxemia and respiratory alkalosis initially, followed by respiratory acidosis. Nursing Management the nurse constantly monitors the patient for the first 12 to 24 hours, or until status asthmaticus is under control. Fluid intake is essential to combat dehydration, to loosen secretions, and to facilitate expectoration.
The pulmonary artery catheter muscle relaxant pain reliever cheap imitrex 50 mg with visa, described in greater Nursing Interventions Patients receive nothing to eat or drink for 8 hours before the procedure muscle relaxant jaw pain quality 50 mg imitrex. The physician threads a singlelumen or multilumen catheter through the external jugular spasms calf buy cheap imitrex 25 mg on line, antecubital muscle relaxant metaxalone side effects cheap imitrex 100 mg buy, or femoral vein into the vena cava just above or within the right atrium. Catheter placement is confirmed by a chest x-ray, and the site is inspected daily for signs of infection. The dressing and pressure monitoring system or water manometer are changed according to hospital policy. The airfluid interface of the stopcock of the transducer, or the zero mark on the manometer, must be level with this axis for accurate measurements. When moving from the flat to erect positions, the patient moves the chest and therefore the reference level; the phlebostatic level stays horizontal through the same reference point. The system can be referenced by placing the airfluid interface of either the in-line stopcock or stopcock on top of the transducer at the phlebostatic level. Pulmonary artery pressure monitoring is achieved by using a pulmonary artery catheter and pressure monitoring system. Catheters vary in their number of lumens and their types of measurement (eg, cardiac output, oxygen saturation) or pacing capabilities. All types require that a balloon-tipped, flow-directed catheter be inserted into a large vein (usually the subclavian, jugular, or femoral vein); the catheter is then passed into the vena cava and right atrium. In the right atrium, the balloon tip is inflated, and the catheter is carried rapidly by the flow of blood through the tricuspid valve, into the right ventricle, through the pulmonic valve, and into a branch of the pulmonary artery. When the catheter reaches a small pulmonary artery, the balloon is deflated and the catheter is secured with sutures. Fluoroscopy may be used during insertion to visualize the progression of the catheter through the heart chambers to the pulmonary artery. This procedure can be performed in the operating room or cardiac catheterization laboratory or at the bedside in the critical care unit. If a thermodilution catheter is used, the cardiac output can be measured and systemic vascular resistance and pulmonary vascular resistance can be calculated. Normal pulmonary artery pressure is 25/9 mm Hg, with a mean pressure of 15 mm Hg (see. When the balloon tip is inflated, usually with 1 mL of air, the catheter floats farther out into the pulmonary artery until it becomes wedged. This is an occlusive maneuver that impedes blood flow through that segment of the pulmonary artery. A pressure measurement, called pulmonary artery wedge pressure, is taken within seconds after wedging of the pulmonary artery catheter; then the balloon is immediately deflated and blood flow is restored. The nurse who obtains the wedge reading ensures that the catheter has returned to its normal position in the pulmonary artery by evaluating the pulmonary artery pressure waveform. The pulmonary artery diastolic reading and the wedge pressure reflect the pressure in the ventricle at end-diastole and are particularly important to monitor in critically ill patients, because they are used to evaluate left ventricular filling pressures (preload). At end-diastole, when the mitral valve is open, the wedge pressure is the same as the pressure in the left atrium and the left ventricle, unless the patient has mitral valve disease or pulmonary hypertension. Critically ill patients usually require higher left ventricular filling pressures to optimize cardiac output. These patients may need to have their wedge pressure maintained as high as 18 mm Hg. Complications of pulmonary artery pressure monitoring include infection, pulmonary artery rupture, pulmonary thromboembolism, pulmonary infarction, catheter kinking, dysrhythmias, and air embolism. A transducer is attached, and pressures are measured in millimeters of mercury (mm Hg). Complications include local obstruction with distal ischemia, external hemorrhage, massive ecchymosis, dissection, air embolism, blood loss, pain, arteriospasm, and infection. Arterial catheters are also useful when arterial blood gas measurements and blood samples need to be obtained frequently. Once an arterial site is selected (radial, brachial, femoral, or dorsalis pedis), collateral circulation to the area must be confirmed before the catheter is placed. This is a safety precaution to prevent compromised arterial perfusion to the area distal to the arterial catheter insertion site.
Imitrex 50 mg buy cheap. Succinylcholine.
Prompt intervention is critical; this includes raising the feet and legs above the head 2410 muscle relaxant purchase imitrex 25 mg otc, administering intravenous fluids muscle relaxant 1 discount 50 mg imitrex amex, and administering intravenous atropine spasms with stretching imitrex 50 mg buy lowest price. Inform the patient that if the procedure is performed percutaneously through the femoral artery (and without the use of devices such as VasoSeal infantile spasms 2 month old order imitrex 50 mg visa, Perclose, or Angio-Seal), the patient will remain on bed rest for 2 to 6 hours with the affected leg straight and the head elevated to 30 degrees (Logemann et al. For comfort, the patient may be turned from side to side with the affected extremity straight. If the cardiologist uses deployed devices, check local nursing care standards, but anticipate that the patient will have less restrictions on elevation of the head of the bed and will be allowed to ambulate in 2 hours or less (Baim et al. Instruct the patient to report chest pain and bleeding or sudden discomfort from the catheter insertion sites immediately. Ensure safety by instructing the patient to ask for help when getting out of bed the first time after the procedure, because orthostatic hypotension may occur and the patient may feel dizzy and lightheaded. For patients being discharged from the hospital on the same day as the procedure, additional instructions are provided. Right Heart Catheterization Right heart catheterization usually precedes left heart catheterization. It involves the passage of a catheter from an antecubital or femoral vein into the right atrium, right ventricle, pulmonary artery, and pulmonary arterioles. Pressures and oxygen saturations from each of these areas are obtained and recorded. Although right heart catheterization is considered a relatively safe procedure, potential complications include cardiac dysrhythmias, venous spasm, infection of the insertion site, cardiac perforation, and, rarely, cardiac arrest. Left Heart Catheterization Left heart catheterization is performed to evaluate the patency of the coronary arteries and the function of the left ventricle and the mitral and aortic valves. Left heart catheterization is performed by retrograde catheterization of the left ventricle. In this approach, the physician usually inserts the catheter into the right brachial artery or a femoral artery and advances it into the aorta and left ventricle. After the procedure, the catheter is carefully withdrawn and arterial hemostasis is achieved using manual pressure or other techniques previously described. If the physician performed an arterial or venous cutdown, the site is sutured and a sterile dressing is applied. If catheterization is to be performed as an outpatient procedure, explain that a friend, family member, or other responsible person must transport the patient home. Prepare the patient for the expected duration of the procedure; indicate that it will involve lying on a hard table for less than 2 hours. Reassure the patient that mild sedatives or moderate sedation will be given intravenously. Explain that an occasional pounding sensation (palpitation) may be felt in the chest because of extrasystoles that almost always occur, particularly when the catheter tip touches the myocardium. The patient may be asked to cough and to breathe deeply, especially after the injection of contrast agent. Coughing may help to disrupt a dysrhythmia and to clear the contrast agent from the arteries. Breathing deeply and holding the breath helps to lower the diaphragm for better visualization of heart structures. Ensure that the patient understands the reason for the study and is able to describe the common sensations and experiences expected during and after the study. In addition, the nurse assists the patient to maintain bed rest with the affected extremity kept straight and the head of the bed elevated to 30 degrees for 4 to 6 hours. The frequency of assessments and the duration of bed rest may vary based on institutional policy and physician preference. Catheters with recording and electrical stimulating (pacing) capabilities are inserted into the heart through the femoral and right subclavian veins to record electrical activity in the right and left atrium, bundle of His, and right ventricle. If the dysrhythmia is induced, various antiarrhythmic medications are administered intravenously. The study is repeated after each medication to evaluate which medication or combination of medications is most effective in controlling the dysrhythmia. After the study, the patient receives an equivalent oral antiarrhythmic agent, and subsequent studies may be necessary to evaluate the effectiveness of that medication. Results of the study may indicate the need for other therapeutic interventions, such as a pacemaker or implantable cardioverter defibrillator. Possible complications include bleeding and hematoma from the catheter insertion sites, pneumothorax (air in the pleural cavity that may collapse portions of the lung), deep vein thrombosis, stroke, and sudden death.
Describe the significance of continuity of care from the health care facility to the home or extended care facility for patients who need rehabilitative assistance and services spasms from catheter imitrex 25 mg order fast delivery. The rehabilitation process helps the patient achieve an acceptable quality of life with dignity muscle relaxant prescriptions imitrex 25 mg visa, self-respect muscle relaxant reviews generic imitrex 50 mg without prescription, and independence and is designed for people with physical quinine spasms discount 25 mg imitrex visa, mental, or emotional disabilities. During rehabilitation-sometimes called habilitation-the patient adjusts to the disability by learning how to use resources and to focus on existing abilities. Rehabilitation is an integral part of nursing because every major illness or injury carries the threat of disability or impairment, which involves a loss of function or an abnormality. The principles of rehabilitation are basic to the care of all patients, and rehabilitation efforts should begin during the initial contact with a patient. If this is not possible, the aims of rehabilitation are maximal independence and a quality of life acceptable to the patient. Realistic goals based on individual patient assessment are established with the patient to guide the rehabilitation program. Rehabilitation services are required by more people than ever before because of advances in technology that save or prolong the lives of seriously ill, injured, and disabled patients. Increasing numbers of patients who are recovering from serious illnesses or injuries are returning to their homes and communities with ongoing needs. Every patient, regardless of age, gender, ethnic group, socioeconomic status, or diagnosis, has a right to rehabilitation services (Chart 11-1). Approximately 1 in 5 Americans has some form of disability, and 1 in 10 has a severe disability (U. A person is considered to have a disability, such as a restriction in performance or function in everyday activities, if he or she has difficulty talking, hearing, seeing, walking, climbing stairs, lifting or carrying objects, performing activities of daily living, doing school work, or working at a job. A severe disability is present if a person is unable to perform one or more activities, uses an assistive device for mobility, or needs help from another person to accomplish basic activities. Individuals are also considered severely disabled if they receive federal benefits based on an inability to work. Approximately 54 million Americans are affected by some form of disability, and this number is expected to increase in the coming decades due to the aging of the population. More than half of R Chapter 11 Principles and Practices of Rehabilitation 159 Chart 11-1 Ethics and Related Issues Are All Persons Entitled to Rehabilitation? Situation You work in an area where many illegal aliens and uninsured residents live. Community violence often creates life-threatening and disabling conditions in members of the population. After a victim of violence has been saved and stabilized, the health care team identifies rehabilitation needs. Dilemma As a health care provider, you are concerned about the community as a whole; costs to the community, and the values of the community. You are also aware of client fiduciary responsibility; you recognize costs to your patient when treatment is provided or not provided. About 5 million persons use a cane, more than 2 million use a wheelchair, and at least 1 million use crutches or a walker. Use of these devices and other types of assistive technology has increased dramatically due to the aging of the population, technological advances, public policy initiatives, and changes in the delivery and financing of health care (U. Disabilities represent disturbances at the level of the person (eg, bathing, dressing, communication, walking, grooming). The employed person with disability, however, earns less money than the nondisabled person (U. Employers must also make "reasonable accommodations," such as equipment or access ramps, to facilitate employment of a person with a disability. Public facilities (eg, stores, restaurants, hotels) must be accessible and accommodate those with disabilities. Although the regulations took effect in July 1992, compliance has been slow because the reasonable accommodation "without undue hardship" provisions in the law permit businesses to continue with inaccessible conditions. All new construction and modifications of public facilities, however, must address access by people with disabilities. Right to Access to Health Care and Health Promotion For years, people with disabilities have been discriminated against in employment, public accommodations, and public and private services including health care.
References
- Miller BJ, Lynch CF, Buckwalter JA. Conditional survival is greater than overall survival at diagnosis in patients with osteosarcoma and Ewing's sarcoma. Clin Orthop Relat Res 2013;471(11):3398-3404.
- Mouthon L. [Causes and mechanisms of systemic vasculitides]. Rev Prat 2008;58(5):487-91.
- Goldberg RJ, Burchfiel CM, Benfante R, et al. Lifestyle and biologic factors associated with atherosclerotic disease in middleaged men: 20-year findings from the Honolulu Heart Program. Arch Intern Med 1995;155:686.
- Lebek G, Cottier H: Notes on the bacterial content of the gut, Curr Stud Hematol Blood Transfus 59:1-18, 1992.
- Craske MG, Barlow DH. Nocturnal panic. J Nervous Mental Dis 1989;177:160-7.