
Regalis
10 mg regalis buy with mastercard
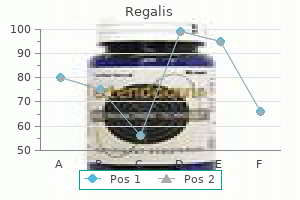
Summary of rationale for recommendations K K K K K K K the risk of fractures after kidney transplant is high erectile dysfunction kidney transplant cheap 5 mg regalis mastercard. J A small study of calcitriol showed worsened bone turnover erectile dysfunction pills supplements regalis 20 mg buy online, but improved mineralization erectile dysfunction systems cheap regalis 10 mg online. J A small study of treatment with bisphosphonates showed worsened bone turnover and mineralization erectile dysfunction protocol free ebook discount regalis 5 mg free shipping. Hypophosphatemia occurs in a large proportion of patients immediately after transplantation, but once kidney function has become stabilized, serum phosphorus returns to the normal range in most of them. Serum calcium tends to increase after transplant and then stabilizes at the higher end of the normal range within 2 months. Post-transplant bone disease represents an important complication observed in a substantial proportion of patients. On the basis of a few bone biopsy studies in transplant patients, glucocorticoids seem to be the primary determinant of subsequent bone volume and turnover. Currently, only one preliminary study is available, suggesting that the progression of cardiovascular calcification may be halted after renal transplantation. The evidence matrix, a table that describes the methodologic quality of the included studies, and the evidence profile, a table that provides an overall assessment of the quality of the evidence and balance of potential benefits and harm are Tables 40, 41 for calcitriol or vitamin D analogs; and Tables 42, 43 for bisphosphonates. Hypercalcemia was present in 40% of recently transplanted recipients and 25% of long-term patients. Hypophosphatemia was very common in the immediate post-transplant period, but normalized within the first year in most series, although a urinary phosphate leak often remained despite normal serum levels. During the first week after kidney transplantation, serum levels of calcium and phosphorus should be measured at least weekly. Many, if not most, kidney transplant recipients develop persistently low levels of serum phosphorus (o3. With a new kidney, there will now be enhanced renal reabsorption of calcium and hypercalcemia may ensue. Thus, during the immediate post-transplant period, wide fluctuations of serum calcium and phosphorus may be seen and thus frequent monitoring is needed. Thus, disorders of mineral metabolism may persist many years after transplantation. Similarly, those with the highest quintile of calcium also had increased risk of kidney allograft loss, which is similar to other reports in which hypercalcemia was associated with both graft loss and recipient death. Increased serum calcium concentration can persist for years after transplantation. Parathyroid gland hyperplasia, especially autonomous parathyroid growth, does not easily resolve after establishment of sufficient renal function, except in mild cases or when secondary to vitamin D deficiency. However, given the magnitude of vitamin D deficiency and the high prevalence of many of the disorders associated with vitamin D deficiency in the general population, the Work Group felt that it was reasonable to treat deficiency, if found. Thus, supplementation with either ergocalciferol or cholecalciferol is recommended, but the optimal treatment regimen is not known,462 and neither is the sufficient level of calcidiol well defined (see Chapter 3. It is also important to point out that the primary source of vitamin D is sunlight, and that the increased risk of skin cancer in kidney transplant patients mandates the use of appropriate sun-screen protection, further increasing the need for oral intake of vitamin D. Thus, vitamin D deficiency is common after transplant, and an initial assessment of status is reasonable. It includes systemic and local derangements of bone and mineral metabolism that can be detected and treated appropriately. Thus, the studies from the general population and other solid organ transplantation may not be generalizable to the kidney transplant population. In addition, there are no treatments in these patients that show fracture reduction (see Recommendation 5. The study found a moderate beneficial effect of vitamin D plus calcium vs no therapy or vs calcium alone (nine trials: effect size 0.
Syndromes
- Agitation
- Chest CT scan (in certain cases)
- Nuclear scan of kidneys
- Hematoma (blood accumulating under the skin)
- Changes in birth control pills or hormone medications
- Apathy
Cheap 10 mg regalis overnight delivery
Thus discount erectile dysfunction pills 10 mg regalis for sale, SkQs look promising as potential tools for treatment of senescence and age-related diseases [31] erectile dysfunction caused by performance anxiety cheap 2.5 mg regalis with visa. The biomarkers of oxidative damage and antioxidative enzyme activity were determined erectile dysfunction at age 23 discount regalis 2.5 mg buy online. It is now apparent that the mitochondrial genome is a weak link in the defenses of ocular cells since it is susceptible to oxidative damage and it lacks some of the systems that protect the nuclear genome erectile dysfunction diabetes buy regalis 2.5 mg without prescription, such as nucleotide excision repair. Accumulation of mitochondrial mutations leads to cellular dysfunction and increased susceptibility to adverse events which contribute to the pathogenesis of numerous sporadic and chronic disorders in the eye [35]. In the anterior segment of the eye, oxidative stress has been linked to lens cataract and glaucoma while in the posterior segment of the eye oxidative stress has been associated with macular degeneration. Consequently, the mitochondria have evolved a number of antioxidant and key repair systems to limit the damaging potential of free oxygen radicals and to repair damaged proteins. The data suggest that these disruptions were globules, vacuoles, multilamellar membranes and clusters of highly undulating membranes. Deleterious structural damage of the lens fibre cell plasma membranes serve as the primary light-scattering centres that cause the observed lens opacity. Phospholipid molecules modified by oxygen accumulate in the lipid bilayer, change its geometry and impair lipid-lipid and protein-lipid interactions in lenticular fibre membranes. The method was applied to determine the pharmacokinetic parameters and the time-course of N-acetylcarnosine and L-carnosine-related product in the eye, following a single dosage of topical ocular administration of peptide. This formulation increases the intraocular absorption of L-carnosine in the aqueous humour and optimises its specific antioxidant activity in vivo while reducing the toxic effects of lipid peroxides on the crystalline lens. The presence of L-carnosine in transparent crystalline lenses during normal aging was detected and its concentration in this case was about 25 microM. At different stages of cataract development, the level of L-carnosine drastically decreased, reaching about 5 microM in ripe human cataracts. These involutions frequently originated near open gaps in the surface epithelia, where they appear to have detached from the capsular membrane. Hasegawa T, Amako H, Yamamoto T, Tazawa M, Sakamoto Y (2014) Corneal-protective effects of an artificial tear containing sodium hyaluronate and castor oil on a porcine short-term dry eye model. Kinetic, Pharmacological and Activity-Dependent Separation of Therapeutic Targeting: Transcorneal Penetration and Delivery of L-Carnosine in the Aqueous Humor and Hormone-Like Hypothalamic Antiaging Effects of the Instilled OphthalmicDrug Through a Safe Eye Medication Technique. Gupta H, Jain S, Mathur R (2007) Sustained ocular drug delivery from a temperature and pH triggered novel in situ gel system. Urtti A (2006) Challenges and obstacles of ocular pharmacokinetics and drug delivery. The objective of an effective therapeutic approach for autoimmune disease is to restore this balance. Taken together, these findings suggest that functionally impaired Treg cells and increased numbers of autopathogenic Th17 cells contribute to the break in tolerance and shift of the immune system towards a proinflammatory state. Treg cells express the transcription factor Foxp3, which is not only a lineage specification factor but also a functional marker of Treg cells. Th17 cell development is a dichotomous process that is regulated through a complex cytokine network. T-bet is also critical for Treg cell homeostasis and function during the Th1 response. Cellular & Molecular Immunology Interplay of Th and Treg cells Leung et al 187 in vivo will create opportunities for the development of therapeutic approaches, including anticytokine therapies that could be used to treat human autoimmune diseases. Critical regulation of early Th17 cell differentiation by interleukin-1 signaling. Interleukins 1beta and 6 but not transforming growth factor-beta are essential for the differentiation of interleukin 17-producing human T helper cells. The interleukin 23 receptor is essential for the terminal differentiation of interleukin 17-producing effector T helper cells in vivo. X-linked neonatal diabetes mellitus, enteropathy and endocrinopathy syndrome is the human equivalent of mouse scurfy. Disruption of a new forkhead/winged-helix protein, scurfin, results in the fatal lymphoproliferative disorder of the scurfy mouse. Molecular antagonism and plasticity of regulatory and inflammatory T cell programs. All-trans retinoic acid mediates enhanced Treg cell growth, differentiation, and gut homing in the face of high levels of co-stimulation. Instability of the transcription factor Foxp3 leads to the generation of pathogenic memory T cells in vivo.
Purchase regalis 10 mg fast delivery
Safeguards should be incorporated to prevent excessive use of tests in patients for whom they have no clinical relevance how young can erectile dysfunction start regalis 10 mg with visa. Limitations Because of significant specimen to specimen collagen crosslink physiologic variability (15-20%) erectile dysfunction 5x5 regalis 10 mg on-line, current recommendations for appropriate utilization include: one or two base-line assays from specified urine collections on separate days; followed by a repeat assay about 3 months after starting anti-resorptive therapy; followed by a repeat assay in 12 months after the 3-month assay; and thereafter not more than annually erectile dysfunction treatment perth generic regalis 5 mg on-line, unless there is a change in therapy in which circumstance an additional test may be indicated 3 months after the initiation of new therapy doctor's advice on erectile dysfunction discount regalis 2.5 mg on line. Urinary N-Telopeptide levels discriminate normal, osteopenic, and osteoporotic bone mineral density. The convenience of the meter or stick color method allows a patient to have access to blood glucose values in less than a minute or so and has become a standard of care for control of blood glucose, even in the inpatient setting. Gestational [pregnancy-induced] hypertension without significant proteinuria, complicating O13. Type I occipital condyle fracture, left side, initial encounter for open fracture S02. Fracture of orbital floor, unspecified side, initial encounter for open fracture S02. Fracture of unspecified part of body of right mandible, initial encounter for closed fracture S02. Fracture of unspecified part of body of left mandible, initial encounter for open fracture S02. Fracture of condylar process of right mandible, initial encounter for closed fracture S02. Fracture of condylar process of right mandible, initial encounter for open fracture S02. Fracture of condylar process of left mandible, initial encounter for open fracture S02. Fracture of subcondylar process of mandible, unspecified side, initial encounter for closed S02. Fracture of coronoid process of mandible, unspecified side, initial encounter for closed S02. Fracture of coronoid process of mandible, unspecified side, initial encounter for open S02. Fracture of coronoid process of right mandible, initial encounter for closed fracture S02. Fracture of coronoid process of left mandible, initial encounter for closed fracture S02. Fracture of ramus of mandible, unspecified side, initial encounter for closed fracture S02. Fracture of ramus of mandible, unspecified side, initial encounter for open fracture S02. Fracture of angle of mandible, unspecified side, initial encounter for closed fracture S02. Fracture of other specified skull and facial bones, unspecified side, initial encounter for S02. Fracture of other specified skull and facial bones, right side, initial encounter for closed S02. Unspecified physeal fracture of right calcaneus, initial encounter for closed fracture S99. Salter-Harris Type I physeal fracture of right calcaneus, subsequent encounter for fracture S99. Salter-Harris Type I physeal fracture of left calcaneus, initial encounter for closed fracture S99. Unspecified physeal fracture of unspecified metatarsal, initial encounter for closed fracture S99. Unspecified physeal fracture of unspecified metatarsal, initial encounter for open fracture S99. Salter-Harris Type I physeal fracture of right metatarsal, initial encounter for open fracture S99. Other physeal fracture of left metatarsal, initial encounter for closed fracture S99.
Generic 5 mg regalis free shipping
The lowest rank of evidence (C) is assigned when expert consensus is the primary basis for the recommendation erectile dysfunction specialist purchase regalis 5 mg without prescription. Symptoms are usually transient erectile dysfunction vacuum pump demonstration regalis 10 mg buy cheap, worse with prolonged reading or watching television because of decreased blinking erectile dysfunction trimix regalis 20 mg purchase without prescription. Symptoms are worse in dry erectile dysfunction needle injection regalis 10 mg free shipping, cold, and windy environments because of increased evaporation. Penlight Examination Findings Bilateral redness Blepharitis Uveitis Redness greater at the margins of eyelids Decreased vision, poorly reacting pupils, constant eye pain radiating to temple and brow. Appearance of a hazy/steamy cornea, moderately dilated pupils that are unreactive to light. Relying on the type of discharge and patient symptoms does not always lead to an accurate diagnosis. Thirty-six percent of conjunctivitis cases are due to adenoviruses, and one study estimated that in-office rapid antigen testing could prevent 1. Evidence-Based Recommendations in Conjunctivitis Recommendation Level of Evidence A19 A41 Herpes Conjunctivitis Herpes simplex virus comprises 1. The discharge is thin and watery, and accompanying vesicular eyelid lesions may be present. Topical and oral antivirals are recommended (Table 2) to shorten the course of the disease. Observation is reasonable in most cases of bacterial conjunctivitis (suspected or confirmed) because they often resolve spontaneously and no treatment is necessary. Bacterial cultures can be useful in cases of severely purulent conjunctivitis or cases that are recalcitrant to therapy. It is often caused by Neisseria gonorrhoeae and carries a high risk for corneal involvement and subsequent corneal perforation. Signs and symptoms include red eye, purulent or mucopurulent discharge, and chemosis (Figure 3). Initial therapy for acute nonsevere bacterial conjunctivitis is listed in Table 2. Antibiotic therapy should be considered in cases of purulent or mucopurulent conjunctivitis and for patients who have distinct discomfort, who wear contact lenses,14,18 who are immunocompromised, and who have suspected chlamydial and gonococcal conjunctivitis. Special Topics in Bacterial Conjunctivitis Methicillin-Resistant S aureus Conjunctivitis At least 60% of cases of suspected or culture-proven acute bacterial conjunctivitis are self-limiting within 1 to 2 weeks of presentation. In a large systemic review, they were found to be effective at increasing both the clinical and microbiological cure rate in the group of patients with culture-proven bacterial conjunctivitis, whereas only an improved microbial cure rate was observed in the group of patients with clinically suspected bacterial conjunctivitis. No data support the use of topical antibiotic therapy in addition to systemic treatment. There are no significant differences in achieving clinical cure between any of the broad-spectrum topical antibiotics. Late complications such as scarring of the eyelid, conjunctiva, and cornea may lead to loss of vision. Patients may also be treated with topical antibiotic ointments for 6 weeks (ie, tetracycline or erythromycin). Systemic antibiotics other than azithromycin, such as tetracycline or erythromycin for 3 weeks, may be used alternatively. Ominous Signs As recommended by the American Academy of Ophthalmology,16 patients with conjunctivitis who are evaluated by nonophthalmologist health care practitioners should be referred promptly to an ophthalmologist if any of the following develops: visual loss, moderate or severe pain, severe purulent discharge, corneal involvement, conjunctival scarring, lack of response to therapy, recurrent episodes of conjunctivitis, or history of herpes simplex virus eye disease. In addition, the following patients should be considered for referral: contact lens wearers, patients requiring steroids, and those with photophobia. Steroids can increase the latency of the adenoviruses, therefore prolonging the course of viral conjunctivitis. In a large systemic review, both antihistamines and mast cell stabilizers were superior to placebo in reducing the symptoms of allergic conjunctivitis; researchers also found that antihistamines were superior to mast cell stabilizers in providing short-term benefits. Therefore, the above causes should be considered in patients presenting with conjunctivitis. Role of the Sponsor: the sponsors played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Cheap regalis 10 mg free shipping
This highest point of the cornea erectile dysfunction drugs gnc cheap regalis 5 mg amex, which indicates a loose superioris not always at the center of the inferior meridian erectile dysfunction after radiation treatment for rectal cancer 2.5 mg regalis with visa, allowing the lens erectile dysfunction aafp discount regalis 20 mg. Lastly causes of erectile dysfunction in youth trusted regalis 2.5 mg, toric peripheral curve the entire lens chamber or just at systems can improve scleral lens the central area. The second option is with rewards that far outweigh to adjust the angle at which the the required effort. Critical measurements to improve peripheral cornea, the patient may scleral lens fitting. Change in over-refraction after scleral lens settling One indication for adding a on average corneas. This common issue can cause suboptimal or "cloudy" vision, diminished lens comfort and increased chair time and cost for both the patient and practitioner. The contact angle is the angle formed when a drop of liquid is placed on a surface. Low-melt wax is recommended for gas permeable materials due to the polymers being sensitive to heat that could impact the on-eye performance of the material. Even with an ideal scleral lens fit and a thorough lens care regimen, fogging may still occur. Factors that have been linked to scleral fogging include increased accumulation of tear debris in the lens reservoir, minimal tear exchange, increased mucin production from conjunctival tissue rubbing, accumulation of protein and lipid deposits on the front surface of the lens and corneal edema. The first strategy to improve surface wettability in scleral lens patients is simply lens removal, manual cleaning to eliminate deposits (and improve the lens surface), rinsing and reapplication. Using preservative-free artificial tears throughout the day to increase lubrication over the lens may also be beneficial. If ocular surface disease is not properly managed, the scleral lens surface may continue to be compromised despite changes in lens material and designs. Dietary changes such as omega fatty acid supplementation and reducing fried and fatty foods may help reduce anterior surface debris by creating a more stable and healthier tear film. This results in a decreased (and thus improved) wetting angle, surface tension and deposition of lipids, proteins and bacteria. When dealing with this issue, it is first important to distinguish between anterior surface fogging and post-lens tear reservoir fogging. A scleral lens with front surface debris, as seen here, could cause wettability issues or fogging, both of which complicate comfortable lens wear. If this is present, scleral lens removal and reapplication will not resolve symptoms-instead, the patient needs medical management for the underlying condition. In these cases, scleral lens wear may need to be discontinued completely or may be worn on a limited wear basis. Instruct patients to monitor how many hours scleral lenses are worn prior to experiencing hazy vision or rainbows around lights. If issues with meibomian reapplying the lens, cleaning the surface deposits, and according debris persist, try removing and lens with an enzymatic cleaner or to the Scleral Lenses in Current reapplying the lens. Another option is Menicon Progent, a chemical biweekly cleaner with a 30-minute soak. It consists of a 90% water polyethylene glycol-based polymer mixture that permanently encapsulates the lens. Patients should be instructed to clean their lenses daily with a multi-purpose or hydrogen peroxide solution and to avoid tap water and abrasive or alcohol-based solutions. S cleral lenses can be a great option for any number of patients, even if wettability and fogging enter the clinical picture. These management strategies, along with proper lens care, can go a long way to ensure healthy life-long scleral lens wear for your patients. Applicability of contact angle techniques used in the analysis of contact lenses, part 1: comparative methodologies. The application of low-temperature plasma technology on the surface modification of biomaterials.
Lesser Cardamom (Cardamom). Regalis.
- What is Cardamom?
- Dosing considerations for Cardamom.
- Are there safety concerns?
- How does Cardamom work?
- Intestinal spasms, heartburn, irritable bowel syndrome (IBS), cold, cough, bronchitis, inflammation of the mouth and throat, liver and gallbladder problems, loss of appetite, preventing infections, gas, constipation, and urinary problems.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96609
5 mg regalis order overnight delivery
The initial multifocal power was the spherical equivalent of a standardized subjective refraction erectile dysfunction injections australia discount 10 mg regalis fast delivery, rounded to the nearest 0 erectile dysfunction pills philippines generic regalis 20 mg online. Over 60 optometrists and other eye care providers erectile dysfunction levitra purchase regalis 5 mg with mastercard, as well as representatives from most major contact lens manufacturers erectile dysfunction treatment for diabetes discount 20 mg regalis otc, attended the workshop. Other verification requests were made and filled, even when inadequate follow-up or no follow-up was performed. As such, this topic deserves attention, and hopefully new technology can ease the burden of this process. The rule would also require prescribers to keep the signed document on file for at least three years. It is a sterile, buffered isotonic saline solution that can be used to rinse soft and gas permeable lenses. However, manufacturers continue to introduce new designs that make these lenses a potentially helpful option for healthy eyes with hyperopia, myopia, astigmatism and presbyopia. These lenses also provide good vision stability due to lack of rotation and minimal movement with blink. Scleral lenses are filled with fluid, which provides constant ocular surface hydration, meaning they cause fewer factors related to lens-induced discomfort compared with soft lenses. Additionally, the larger optic zone provides minimal halos and glare, resulting in enhanced vision. Of the 84,375 patients represented in the study, only 70 cases of microbial keratitis were reported. Results from this study suggest that vision-threatening complications associated with scleral lens wear may be rare. Because soft lenses rely on rotational stability for clear vision, lens rotation while blinking can result in vision fluctuation during the day. If this occurs, patients often feel they are compromising their vision to wear contact lenses. One recent study reports scleral lenses as a viable alternative to soft toric lenses for astigmatic subjects. Subjects wore each modality for one month, with 75% preferring the vision of the scleral lenses compared with the soft toric lenses, and 53% expressing a preference to continue with the scleral modality. Scleral lenses also feature an 8mm to 9mm optic zone, which enhances the field of vision and limits interaction with the pupil diameter and the perception of higher-order aberrations. To resolve this, practitioners can incorporate toric haptics to achieve a better lens alignment in all quadrants. Additionally, these lenses compensate for high degrees of refractive astigmatism without the need for a front surface toric design. Currently, there are questions about how the combination of lens material, lens thickness and post-lens tear reservoir affect corneal physiology. Various studies have suggested that, despite the availability of highly breathable materials, hypoxia is still a concern. Due to his high degree of hyperopic and astigmatic correction, he was self-conscious about wearing glasses at school. He reported the magnification of his eyes made students stare and he felt they could notice his eyes shake. He also reported improvement in the quality of his vision and felt more confident at school while wearing his contact lenses. Lens manufacturers and educational aids, such as the Scleral Lens Education Society, can help guide practitioners to provide successful lens fits for all patients. Acute red eye (non-ulcerative keratitis) associated with mini-scleral contact lens wear for keratoconus. This start-up guide can help you learn how best to approach a scleral lens fitting. At the top of the list is the fluid layer created between the cornea and back surface of the lens. The fluid layer also bathes the entire cornea during lens wear, while the large lens size protects the ocular surface from environmental agents, eyelid friction and air exposure. The lens sits behind both eyelids, and the large diameter limits interaction with the lens edge, significantly improving comfort for patients that have had trouble tolerating corneal lenses in the past. Also, a properly fit scleral lens does not move much, if at all, further improving comfort. Based on these benefits, patients with irregular corneas make excellent candidates for scleral lenses.
5 mg regalis purchase with visa
Common comorbid psychiatric disorders include mood and anxiety disorders erectile dysfunction doctor in nashville tn buy 2.5 mg regalis otc, substance use disorder erectile dysfunction drugs compared regalis 20 mg lowest price, and intermittent explosive disorder (Bukstein 2018) erectile dysfunction treatment by ayurveda order 5 mg regalis otc. About 30% of patients do not respond to or may not tolerate the initial stimulant treatment erectile dysfunction 40s regalis 2.5 mg buy with amex. At least one-half of children who do not respond to one type of stimulant will respond to the other. Concerta is approved for use in children 6 years of age and older, adolescents, and adults up to 65 years of age. No significant difference was seen in the 25 mg or 70 mg groups compared to placebo. There was no evidence that one kind of amphetamine was better than another and there was no difference between short-acting and long-acting formulations. The 2 classes of stimulant medications did not differ significantly from one another. One small study found that tic severity was significantly increased with higher doses of dextroamphetamine treatment. Methylphenidate is recommended for preschool-aged children who have had an inadequate response to behavioral interventions. Some patients may respond similarly to different stimulant classes, whereas other patients may respond preferentially to only 1 of the classes of stimulants. Mixing short- and long-acting stimulants can be helpful to achieve an immediate effect for early-morning school classes or for reducing rebound irritability or overactivity, especially in the evening. Atomoxetine is an alternative for patients who cannot tolerate stimulants or for whom treatment with a controlled substance is undesirable. It carries a boxed warning for a rare increased risk of suicidal ideation in children and adolescents. The capsules may be swallowed whole or can be opened, emptied, and mixed with yogurt, water, or orange juice and consumed immediately. The capsule may be swallowed whole or it may be opened and the contents sprinkled onto applesauce and given immediately. The capsule contents must not be crushed or chewed, the dose of a single capsule should not be divided, and the contents of the entire capsule should be taken at the same time. A 10 mg or 15 mg dose can be achieved by breaking in half the functionally scored 20 mg and 30 mg tablets, respectively. With twice daily dosing, either an equal or higher split dosage should be given at bedtime. The tablets should not be crushed, chewed, or broken prior to swallowing; they should not be administered with high fat meals, due to increased exposure It may be necessary to reduce the dosage in patients with significant renal and hepatic impairment. Although non-stimulants such as atomoxetine and alpha2-adrenergic agonists have smaller effect sizes, they may be used in patients who have failed or are intolerant to stimulants or when there is concern about possible abuse or diversion. Treatment of attention-deficit/hyperactivity disorder in adolescents: a systematic review. Efficacy, safety, and tolerability of an extended-release orally disintegrating methylphenidate tablet in children 6-12 years of age with attention-deficit/hyperactivity disorder in the laboratory classroom setting. Atomoxetine for attention deficit hyperactivity disorder in the adulthood: a meta-analysis and metaregression. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Psychological, pharmacological, and combined treatments for binge eating disorder: a systematic review and meta-analysis. Alpha-2 agonists for attention-deficit/hyperactivity disorder in youth: a systematic review and meta-analysis of monotherapy and add-on trials to stimulant therapy. Efficacy of lisdexamfetamine in adults with moderate to severe binge-eating disorder: A randomized clinical trial. Comparative efficacy and safety of attention-deficit/hyperactivity disorder pharmacotherapies, including guanfacine extended release: a mixed treatment comparison. Attention deficit hyperactivity disorder in children and adolescents: Treatment with medications. Lisdexamfetamine dimesylate for adults with moderate to severe binge eating disorder: Results of two pivotal phase 3 randomized controlled trials. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin.
Cheap regalis 5 mg online
The field of gene therapy started with a visionary and a daring idea erectile dysfunction jack3d regalis 20 mg overnight delivery, but suffered from a dearth of preclinical data erectile dysfunction treatment mayo clinic purchase regalis 20 mg with mastercard. Through the years erectile dysfunction medications comparison generic 20 mg regalis with mastercard, the field of gene therapy has overcome several crises at the collision of public expectations and unintended side effects erectile dysfunction gabapentin buy 2.5 mg regalis, and has emerged as an acceptable therapy in the treatment of several genetic disorders. Cavazza A, Moiani A, Mavilio F (2013) Mechanisms of retroviral integration and mutagenesis. Good to Know A second primary cancer refers to the presence of an additional, unrelated cancer in someone who was previously diagnosed with another type of cancer. Because a detailed review of head and neck cancer is not feasible in this chapter, we recommend consulting reference textbooks (22 and 23). Therefore, maintenance of proper oral hygiene and routine dental evaluations are recommended. Distinguishing suspicious lesions from those that are non-cancerous requires the input of a health care provider with significant experience in the evaluation and management of head and neck cancer. Appropriate professionals may have dental, oral surgery, otolaryngology, or general surgery backgrounds supplemented with specialized training in head and neck cancer. Examination of the distal oropharynx (the back of the throat), nasopharynx (the uppermost part of the throat, between the nasal cavity and the soft palate), larynx, and hypopharynx (the bottommost part of the throat) requires the use of either a transoral mirror or a flexible fiberoptic laryngoscope. A free flap refers to the transplant of a piece of tissue from one site of the body to another for the reconstruction of a defect. For example, N0 describes a cancer that has not spread to nearby lymph nodes, whereas N1 indicates lymph node involvement. The values for T, N, and M are then combined to assign an overall stage to the cancer. Optimized medically means that a doctor has chosen the best treatment for a patient depending on his or her individual circumstances. A qualified professional should perform a thorough head and neck examination every 6 months. Once a premalignant or malignant lesion has been identified and appropriately treated, the frequency of surveillance examinations should be increased to once every 2-3 months. An experienced examiner should be able to distinguish lesions that need to be biopsied from those that can simply be followed over time. A brush biopsy may be used for screening, but a tissue biopsy is recommended to establish a definitive diagnosis. In general, a wide complete excision of the primary tumor should be performed with adequate margins. The margins for laryngeal tumors need not be as comprehensive, due to the unique anatomy of the larynx. Death may be due to local effects, but systemic effects such as bone marrow failure are also major contributors. Therefore, radiation therapy should only be used in patients for whom it is absolutely required for disease control. If radiation therapy is to be utilized, patients must be optimized medically and monitored closely for signs for severe toxicity. These studies demonstrated an absolute 5-year survival benefit of approximately 6. However, the addition of cytotoxic 279 Fanconi Anemia: Guidelines for Diagnosis and Management chemotherapy to radiation therapy has been associated with an increased incidence of adverse events, including mucositis (inflammation of the mucous membranes), dermatitis (inflammation of the skin), skin toxicities, and the need for feeding tube placement (16). For patients with recurrent/metastatic disease, the cornerstone of treatment is systemic therapy with single agents (cisplatin, taxanes, 5-fluorouracil, or methotraxate), or platinum-based doublet regimens (the combination of a platinum-based drug with other chemotherapy agents) to ease pain. The issue is further complicated by the lack of prospective trials, or even large retrospective series evaluating the safety and efficacy of cytotoxic agents in this patient population. Furthermore, cytotoxic chemotherapy 280 Chapter 14: Head and Neck Cancers in Patients with Fanconi Anemia at both standard and low doses is associated with severe, and in many cases fatal, toxicities and poor treatment outcomes. The patient also developed grade 3 dermatitis (following 50 Gy of radiation therapy), mucositis (following 45 Gy of radiation therapy), and cholestasis, but all were clinically manageable.
Discount 5 mg regalis free shipping
Patients will feel empowered as they gain the skills and confidence to be active participants in their care erectile dysfunction gene therapy treatment order regalis 2.5 mg amex. Peer Educators and Patient Advisory Groups Patients need to be active participants in making decisions regarding their health care erectile dysfunction treatment in egypt 5 mg regalis buy with mastercard. Peer educators and patient advisory groups can help patients become more involved in their care erectile dysfunction treatment psychological regalis 5 mg buy with mastercard. In order to best support patients erectile dysfunction treatment in dubai regalis 20 mg order amex, it is helpful to have peer educators available for them during initial and subsequent visits. This helps to decrease patient anxiety and promotes a patient-centered atmosphere. Positive change in behavior needs to be an ongoing focus of patient-centered care. After patients have selfmanagement skills, they still need help setting action plans for their health care. They should be educated about that, and also taught what to do in situations that do pose risk, such as when bleeding occurs. For example, gloves should be worn only as appropriate during physical examinations and as consistent with universal precautions. Some patients may feel ambivalent about seeking medical care if, by doing so, they risk disclosing their condition. Others may have learned from experience to expect rejection and therefore may not trust care providers. It is essential for providers to be supportive of patients who are dealing with the burden of stigma. Stigma Associated with Being Gay, Lesbian, Bisexual, or Transgender Demonstrating respect and providing excellent care to patients with various cultural backgrounds, beliefs, and sexual orientations are central to medical professionalism. Providers and social workers should be aware of community agencies with resources available to people who are lesbian, gay, or transgender. In addition, providers and clinic staff members should be aware of special legal issues that affect these populations. For example, designating a durable power of attorney for medical decision making can be particularly important in states that do not recognize same-sex partners as legal next of kin. All these obstacles can make accessing health care difficult and attending to health problems less of a priority for the individual. Culturally competent communication between provider and patient may substantially affect adherence with therapies. The team of peer educators should be culturally diverse in order to be effective with all minority groups. Personnel policies should reinforce measures such as requirements that papers and computer screens containing patient-identifying information not be left unattended and should include provisions for documenting whether phone messages can be left for the patient, and if so, with whom. Patients may find support groups or individual psychotherapy sessions beneficial in deciding when to disclose, and to whom. Local health departments can either assist patients in making these disclosures or provide anonymous partner notification for them. Providers should become familiar with the laws of their jurisdiction by contacting their health department. Assure them that their names are always kept confidential and are never given to potentially exposed individuals by the health department. Thus, chronic treatment and retention in care are important for both individuals and public health. At the same time, funding streams from federal, state, and local governments create opportunities for treatment of uninsured and underinsured individuals and provide resources for creating innovative, effective programs. Treatment guidelines, operations research data, and technical support are available to assist in designing, operating, and improving service programs. Patient Recruitment into Clinic the persons who were easy to recruit and retain in care are already enrolled; the more challenging patients await recruitment. However, for the clinics, the numbers of newly diagnosed patients who present for care is substantial. Clinic personnel should build personal relationships with agencies that may provide referrals, invite staff of community agencies to visit the clinic, or hold open houses.
Order 20 mg regalis visa
Information on pregnancy risks and complications-including smoking erectile dysfunction treatment boots order regalis 20 mg with amex, infections erectile dysfunction causes in young men generic regalis 2.5 mg, medications erectile dysfunction suction pump 20 mg regalis buy otc, exposure to X-rays erectile dysfunction medication new zealand order 5 mg regalis with mastercard, occupational history, and exposure to anesthetic gases, ethylene oxide, herbicides, and pesticides-was collected for each pregnancy. For the comparison group, the first pregnancy after July 4, 1965, was designated as the index pregnancy. The study analyzed data on 3,392 Vietnam and 3,038 non-Vietnam veterans and on 1,665 Vietnam and 1,912 nonVietnam veteran index pregnancies. The authors attempted to "retrieve hospital records on all reported cancers as far back as 30 years. The authors did not provide specific data on diagnosis confirmation for the three sites other than the breast, but they stated that Vietnam status was not associated with a greater likelihood of finding confirmatory medical records. The legislation covers 18 birth defects, including cleft lip or palate, congenital heart disease, hypospadias, neural-tube defects, and Williams syndrome. Proportionate-Mortality Cohort Among the earliest reports on health outcomes in Vietnam veterans was a proportionate-mortality study by Breslin et al. The participants were Army and Marine Corps ground troops (all men) who served at any time from July 4, 1965, through March 1, 1973. From this list, 75,617 individuals were randomly selected for inclusion in the study. The information extracted from the selected military records included duty stations, dates of tours, branch of military service, date of birth, sex, race, military occupation specialty codes, education level, type of discharge, and confirmation of service in Vietnam. Additional information was extracted on veterans who served in Southeast Asia, including the first and last dates of service in Southeast Asia, the military unit, and the country where the veteran served. For the final sample of Army and Marine Corps veterans, the cause of death was ascertained from death certificates or Department of Defense (DoD) Report of Casualty forms for 24,235 men who served in Vietnam and 26,685 men who did not serve in Southeast Asia. Exposue to herbicides or other environmental factors was not considered in the analysis. Deaths from external causes (accidents, poisonings, and violence) were slightly eleveated among Vietnam veterans who served in the Army but not among marines who served in Vietnam. Death from any cancer was elevated among marines who served in Vietnam but not Army veterans. Deaths from external causes (accidents, poisonings, and violence) were found to be slightly eleveated among Army I Corps Vietnam veterans, particularly deaths attributed to motor vehicle accidents and accidental poisonings. An additional 11,325 deceased Army and Marine Corps Vietnam-era veterans were identified from the period and included in the study. Proportionate-mortality ratios were calculated for three referent groups: branch-specific (Army and Marine Corps) non-Vietnam veterans, all non-Vietnam veterans combined, and the U. Deaths from external causes were again statistically significantly elevated among Vietnam-deployed marines compared with non-Vietnam veterans and Army veterans who served in Vietnam compared with Army veterans who did not serve in Vietnam and all non-Vietnam veterans. Cancer of the larynx was statistically significantly higher among Vietnam-deployed Army veterans than either non-Vietnam Army veterans or all non-Vietnam veterans but lung cancer was only significantly different for Army Vietnam veterans compared with all non-Vietanm veterans. A third follow-up proportionate-mortality study (Watanabe and Kang, 1996) used the veterans from Breslin et al. The final study included 70,630 veterans-33,833 who had served in Vietnam and 36,797 who had never served in Southeast Asia. Just as in the previous analyses of mortality, Army and Marine Corps Vietnam veterans had statistically significant excesses of deaths from external causes. Army Vietnam veterans had statistically significant excesses of deaths for laryngeal cancer and lung cancer when compared to both Army non-Vietnam veterans and all non-Vietnam veterans. Results showing statistical significance for Marine Corps Vietnam veterans varied according to the referent population used (non-Vietnam marine veterans or all non-Vietnam veterans). Deaths from circulatory diseases were statistically significantly lower among Marine Corps Vietnam veterans than marines who did not serve in Vietnam and all non-Vietnam veterans. Marine Corps Vietnam veterans also had significant excesses for lung cancer and skin cancer compared with all non-Vietnam veterans. Proportionate mortality ratios for deaths due to respiratory and digestive diseases were statistically significantly lower among marine Vietnam veterans than all non-Vietnam veterans. However, cancers overall were higher among the Vietnam-deployed and non-deployed Army veteran groups and the Marine Corps non-Vietnam veteran group.