
Udenafil
Buy udenafil 100 mg low price
In the studies with Nebido particular attention was paid to local tolerability (at the injection site) ketoconazole impotence cheap 100 mg udenafil with visa, to possible effects on the urogenital system erectile dysfunction due to diabetes icd 9 udenafil 100 mg visa, and to special test parameters erectile dysfunction treatment south africa purchase udenafil 100 mg fast delivery. A prospective study examining injection-site pain in men receiving Nebido found gluteal injection to be well tolerated impotence news 100 mg udenafil purchase with mastercard. Pain persisted for only 12 days, with complete resolution by day 4, and few patients required analgesics. Patients who had experienced an earlier painful injection reported increased injection site pain, whereas older and obese patients reported less pain. Nebido Product Monograph 57 Figure 27: Changes in prostate specific antigen levels and prostate volume during long-term treatment with Nebido. The few abnormal findings of clinical significance were not attributable to the treatment with Nebido. Although Nebido is currently contraindicated in patients with prostate cancer, recent guidelines for the management of hypogonadism suggest that testosterone replacement therapy can be used with caution in selected patients who have undergone surgical treatment of prostate cancer at least 1 year earlier when there is no evidence of active disease. These increases were considerably smaller for patients previously treated with a different testosterone product than testosterone-naпve patients, but were comparable for these cohorts at 1 year. In a prospective observational study of 347 patients who received a total of 3,022 injections over a 3. This retrospective study involved 179 men, 162 of whom completed 2 years of treatment. A study conducted in 88 men with late-onset hypogonadism reported corrections in the lipid profile after treatment with Nebido. Studies have shown mild worsening of sleep-disordered breathing in obese men with sleep apnoea treated with Nebido. Nonetheless, physicians administering Nebido should be aware of the potential for serious allergic reactions to its components. Treatment with Nebido produced durable increases in serum testosterone to eugonadal levels for men within 18 weeks. Nebido was well tolerated and the only adverse event reported was a rapid-onset male pattern baldness (occurring in one of seven patients in one study). Glucose parameters and markers of inflammation were also improved from baseline (p<0. The white blood cell count decreased, while haemoglobin and haematocrit increased. The results of this pilot study were confirmed in the long-term follow-up of the same group. Nebido Product Monograph 65 9 Conclusion Nebido represents an innovative formulation for testosterone therapy. Nebido is the first long-acting testosterone preparation for intramuscular injection. Nebido needs to be administered only about 4 times per year for restoration of testosterone levels to the eugonadal range. Unphysiologically high peaks in testosterone levels are largely avoided after the administration of Nebido. Nebido is effective in the treatment of male hypogonadism: · · · · · · improvement in libido and sexual function improvement in haematological parameters improvement in body composition increased muscle strength a positive effect on mind and mood improved metabolic parameters Nebido proved to be very well tolerated. Reactions at the injection site and other side effects specific to testosterone occurred only in individual cases. As with any androgen therapy, the use of Nebido is contraindicated in known cases of carcinoma of the mammary or prostate glands. The prostate and haematological parameters must be regularly monitored during the treatment. Complete androgen insensitivity syndrome: long-term medical, surgical, and psychosexual outcome. Functional cross-talk between the hypothalamic-pituitary-gonadal and -adrenal axes.
Udenafil 100 mg fast delivery
Most episodes of fever in children younger than 3 years of age have a demonstrable source of infection elicited by history hcpcs code for erectile dysfunction pump udenafil 100 mg with mastercard, physical examination erectile dysfunction on coke udenafil 100 mg purchase fast delivery, or a simple laboratory test erectile dysfunction lotion udenafil 100 mg buy visa. Stool culture should be obtained in those with diarrhea marked by blood or mucous psychological erectile dysfunction drugs buy udenafil 100 mg line. Ill-appearing children should be admitted to the hospital and treated with empirical antibiotics. No combination of demographic factors (socioeconomic status, race, gender, and age), clinical parameters, or laboratory tests in these children reliably predicts occult bacteremia. Occult bacteremia in otherwise healthy children is usually transient and self-limited but may progress to serious localizing infections. Admit and treat No Yes Observe or treat Yes No Figure 96-1 Approach to a child younger than 36 Finish evaluation and admit and treat months of age with fever without localizing signs. The specific management varies, depending on the age and clinical status of the child. Regardless of antibiotic treatment, close follow-up for at least 72 hours, including re-evaluation in 24 hours or immediately with any clinical change, is essential. Children with a positive blood culture require immediate re-evaluation, repeat blood culture, consideration for lumbar puncture, and empirical antibiotic treatment. Children with sickle cell disease have impaired splenic function and properdin-dependent opsonization that places them at increased risk for bacteremia, especially during the first 5 years of life. Other children with sickle cell disease and fever should have blood culture, empirical treatment with ceftriaxone, and close outpatient follow-up. It is important to distinguish persistent fever from recurrent or periodic fevers, which usually represent serial acute illnesses. Additional laboratory and imaging tests are guided by abnormalities on initial evaluation. Sinusitis, endocarditis, intra-abdominal abscesses (perinephric, intrahepatic, subdiaphragmatic), and central nervous system lesions (tuberculoma, cysticercosis, abscess, toxoplasmosis) may be relatively asymptomatic. Fever eventually resolves in many of these cases, usually without sequelae, although some may develop definable signs of rheumatic disease over time. Factitious fever or fever produced or feigned intentionally by the patient (Munchausen syndrome) or the parent of a child (Munchausen syndrome by proxy) is an important consideration, particularly if family members are familiar with health care practices (see Chapter 22). Fever should be recorded in the hospital by a reliable individual who remains with the patient when the temperature is taken. Continuous observation over a long period and repetitive evaluation are essential. Consultation with infectious disease, immunology, rheumatic disease, or oncology specialists should be considered. Further tests may include lumbar puncture for cerebrospinal fluid analysis and culture; computed tomography or magnetic resonance imaging of the chest, abdomen, and head; radionuclide scans; and bone marrow biopsy for cytology and culture. Rash distribution and appearance provide important clues to the differential diagnosis, including other infectious agents (Table 97-1). Measles virus infects the upper respiratory tract and regional lymph nodes and is spread systemically during a brief, low-titer primary viremia. A secondary viremia occurs within 5 to 7 days as virus-infected monocytes spread the virus to the respiratory tract, skin, and other organs. Virus is present in respiratory secretions, blood, and the urine of infected individuals. Measles virus is transmitted by droplets or the airborne route and is highly contagious. Infected persons are contagious from 1 to 2 days before onset of symptoms-from about 5 days before to 4 days after the appearance of rash-and immunocompromised persons can have prolonged excretion of contagious virus. Epidemiology Measles remains endemic in regions of the world where measles vaccination is not available and is responsible for about 1 million deaths annually. Since 2000 there typically have been fewer than 100 cases reported annually in the United States, although outbreaks resulting from imported virus after international travel occur. Infections of nonimmigrant children during outbreaks may occur among those too young to be vaccinated or in communities with low immunization rates. Most young infants are protected by transplacental maternal antibody until the end of their first year. Clinical Manifestations Measles infection is divided into four phases: incubation, prodromal (catarrhal), exanthematous (rash), and recovery.
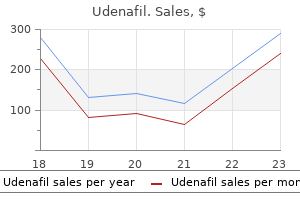
| Comparative prices of Udenafil | ||
| # | Retailer | Average price |
| 1 | Verizon Wireless | 578 |
| 2 | Brinker International | 175 |
| 3 | GameStop | 281 |
| 4 | Publix | 720 |
| 5 | Menard | 962 |
| 6 | AutoZone | 331 |
Buy udenafil 100 mg without a prescription
Suspected cases of vaccine-preventable diseases should be reported to state or local health departments erectile dysfunction treatment mumbai buy udenafil 100 mg otc. The act also established the National Vaccine Injury Compensation Program impotence in the bible buy udenafil 100 mg on line, a no-fault system in which persons thought to have suffered an injury or death as a result of administration of a covered vaccine can seek compensation erectile dysfunction rates cheap udenafil 100 mg otc. Conjugation of a polysaccharide to a protein carrier induces a T-dependent response in infants and creates immunogenic vaccines for H impotence from priapism surgery udenafil 100 mg low price. In the United States, due to state laws requiring immunization for school entry, approximately 95% of children entering kindergarten are vaccinated for the common infectious diseases. This schedule includes up to 21 injections in four to five visits by 18 months of age. Children and adolescents who are at increased risk for pneumococcal infections should receive the pneumococcal polysaccharide vaccine, as well. Children who are behind in immunization should receive catch-up immunizations as rapidly as feasible. Infants born prematurely, regardless of birth weight, should be vaccinated at the same chronologic age and according to the same schedule as full-term infants and children (see. The National Childhood Vaccine Injury Act requires that all health care providers provide parents or patients with copies of Vaccine Information Statements prepared by the Centers for Disease Control and Prevention. The preferred sites for administration are the anterolateral aspect of the thigh in infants and the deltoid region in children and adults. Multiple vaccines can be administered simultaneously at anatomically separate sites (different limbs, or separated by >1 in. Administration of blood products and immunoglobulin can diminish response to live virus vaccines if administered before the recommended interval. General contraindications to vaccination include serious allergic reaction (anaphylaxis) after a previous vaccine dose or to a vaccine component, immunocompromised states or pregnancy (live virus vaccines), and moderate or severe acute illness with or without fever. History of anaphylactic-like reactions to eggs is a contraindication to influenza and yellow fever vaccines, which are produced in embryonated chicken eggs. Prophylaxis is also recommended for contacts who frequently sleep or eat in the same dwelling as the index patient or passengers seated directly next to the index case during airline flights lasting longer than 8 hours. For those who fall behind or start late, provide catch-up vaccination at the earliest opportunity as indicated by the green bars in Figure 94-1. Any dose not administered at the recommended age should be administered at a subsequent visit, when indicated and feasible. Figure 94-1 Recommended immunization schedules for persons ages 0 through 18 years-United States, 2013. If the second dose was administered at least 4 weeks after the first dose, it can be accepted as valid. For children aged 7 through 12 years the recommended minimum interval between doses is 3 months (if the second dose was administered at least 4 weeks after the first dose, it can be accepted as valid); for persons aged 13 years and older, the minimum interval between doses is 4 weeks. Doses following the birth dose · the second dose should be administered at age 1 or 2 months. This dose can count as the adolescent Tdap dose, or the child can later receive a Tdap booster dose at age 1112 years. Vaccination of persons with high-risk conditions: · Hib vaccine is not routinely recommended for patients older than 5 years 6a. Always use this table in conjunction with Figure 94-1 and the footnotes that follow. Persons aged 4 months through 6 years Vaccine Minimum Age for Dose 1 Birth 6 weeks 6 weeks Minimum Interval Between Doses Dose 1 to dose 2 4 weeks 4 weeks 4 weeks 4 weeks age 12 months Dose 2 to dose 3 8 weeks Dose 3 to dose 4 Dose 4 to dose 5 Hepatitis B Rotavirus Diphtheria, tetanus, pertussis 4 weeks 4 weeks 4 weeks if current age is younger than 12 months dose administered at younger than age 12 months and second dose administered at younger than 15 months No further doses needed if previous dose administered at age 15 months or older 6 months 6 months type b 6 weeks No further doses needed or older dose) this dose only necessary for children aged 12 through 59 months who received 3 doses before age 12 months dose) this dose only necessary for children aged 12 through 59 months who received 3 doses before age 12 months or for children at high risk who received 3 doses at any age 6 months minimum age 4 see footnote 13 4 weeks age 12 months Pneumococcal 6 weeks older or current age 24 through 59 months No further doses needed age 24 months or older 4 weeks if current age is younger than 12 months if current age is 12 months or older No further doses needed for healthy children if previous dose administered at age 24 months or older Inactivated poliovirus Meningococcal Measles, mumps, rubella Varicella Hepatitis A 6 weeks 6 weeks 12 months 12 months 12 months 4 weeks 8 weeks 4 weeks 3 months 6 months 4 weeks see footnote 13 Persons aged 7 through 18 years Tetanus, diphtheria; tetanus, diphtheria, pertussis 4 weeks if first dose administered at younger than age 12 months 6 months or older Human papillomavirus Hepatitis A Hepatitis B Inactivated poliovirus Meningococcal Measles, mumps, rubella Varicella 9 years 12 months Birth 6 weeks 6 weeks 12 months 12 months 6 months 4 weeks 4 weeks 8 weeks 4 weeks 3 months if person is younger than age 13 years 4 weeks if person is aged 13 years or older 8 weeks 4 weeks 6 months Routine dosing intervals are recommended 6 months administered at younger than age 12 months 7 years 4 weeks Figure 94-2 Catch-up immunization schedule for persons ages 4 months through 18 years who start late or who are more than 1 month behind-United States, 2013. This figure provides catch-up schedules and minimum intervals between doses for children whose vaccinations have been delayed. Always use this table in conjunction with the Recommended Immunization Schedule for 2013 and the footnotes that follow. Department of Health and Human Services, Centers for Disease Control and Prevention. The final dose in the series should be administered on or after the fourth birthday and at least 6 months after the previous dose.
Trusted udenafil 100 mg
Therefore erectile dysfunction in diabetes management udenafil 100 mg free shipping, patients taking calcineurin inhibitors for more than 1 year may require periodic blood tests and serial kidney biopsies to insure that irreversible kidney injury does not occur xyzal erectile dysfunction buy udenafil 100 mg free shipping. This was confirmed in a study of 54 children (mean age 11 years) in which rituximab plus low-dose steroids and tacrolimus was as effective as treatment with standard doses of the latter two drugs; however erectile dysfunction mental treatment cheap udenafil 100 mg buy online, this therapy is costly erectile dysfunction treatment pdf discount udenafil 100 mg without prescription, and the long-term risks are unknown. Target trough levels for cyclosporine and tacrolimus are 100-200 ng/mL and 4-8 ng/mL, respectively. After achieving remission, reduce doses to the lowest dose compatible with staying in remission. Initial treatment with corticosteroids results in remission of proteinuria in nearly all patients; however, 90% of patients will manifest a frequently relapsing or steroid-dependent course with steroid toxicity. These patients are candidates for treatment with second-line agents such as cyclophosphamide, mycophenolate mofetil, or tacrolimus. The choice of drug will vary from center to center and reflect local experience and preferences of the individual physician. The disease can persist into adulthood and can lead to chronic sequelae such as bone demineralization, atherosclerosis, and obesity. Therefore, long-term follow-up is warranted in those patients who continue to relapse and require immunosuppressive medication. Fakhouri F, Bocqueret N, Taupin P, et al: Children with steroid-sensitive nephrotic syndrome come of age: long-term outcome, J Pediatr 147:202-207, 2005. Kisner T, Burst V, Teschner S, et al: Rituximab treatment for adults with refractory nephrotic syndrome: a single-center experience and review of the literature, Nephron Clin Pract 120:c79-c85, 2012. Kitamura A, Tsukaguchi H, Hiramoto R, et al: A familial childhoodonset relapsing nephrotic syndrome, Kidney Int 71:946-951, 2007. In most patients, relapses are detected by the onset of proteinuria 3 to 4 days before edema ensues. In those patients who develop edema before a relapse is recognized or who respond slowly to prednisone, edema can be controlled by prescribing a low-salt (2 g sodium) diet and oral diuretics. Options include loop diuretics, such as furosemide 1 to 2 mg/kg administered once or twice daily or a thiazide diuretic. The duration of action of diuretic agents may be diminished secondary to hypoalbuminemia and enhanced renal clearance, but this is rarely clinically significant because the medications are only needed for 1 to 2 weeks until treatment response occurs and proteinuria resolves. Children who have frequent relapses and persistent edema are at risk for bacterial peritonitis and can be given prophylactic penicillin. Immunization with the pneumococcal vaccine is also helpful under these circumstances. If feasible, the timing of vaccine administration should be delayed for at least 2 weeks after administration of prednisone to ensure maximal immunologic response. However, this presumed benign course is based on scarce data of patients followed into adulthood. Children who had a relapsing course and/or required immunosuppressive medications were more likely to have persistent disease in adulthood. Zhang L, Dai Y, Peng W, et al: Genome-wide analysis of histone H3 lysine 4 trimethylation in peripheral blood mononuclear cells of minimal change nephrotic syndrome patients, Am J Nephrol 30:505-513, 2009. Gipson that place hemodynamic stress on an initially normal nephron population (as in morbid obesity, cyanotic congenital heart disease, and sickle cell anemia). Consequently, clinicians must carefully assess for potential clinical and pathologic clues with respect to the etiology of this disease. This barrier is composed of the glomerular basement membrane, the podocyte, and the slit diaphragm between the podocytes. Tubular function assists with the recycling of the small amount of proteins that cross the glomerular barrier, maintaining the normal urine protein excretion less than 0. With progressive disease, the podocytes die, subsequently separating from the glomerulus followed by excretion in the urine. When a loss of less than 40% is observed in animal models, limited scarring and mild proteinuria is observed; however, loss of more than 40% of podocytes appears to induce significant scarring and severe proteinuria.
Buy udenafil 100 mg
This reflex is unreliable in neonates except when asymmetrical because the "normal" response at this age varies erectile dysfunction doctors in st. louis udenafil 100 mg buy with mastercard. By 12 to 18 months of age erectile dysfunction drugs prostate cancer purchase 100 mg udenafil with mastercard, the plantar response should consistently be flexor (toes flexing down) erectile dysfunction protocol free 100 mg udenafil buy visa. Excessive muscle bulk is seen in rare conditions erectile dysfunction on prozac discount 100 mg udenafil free shipping, such as myotonia congenita; boys with Duchenne muscular dystrophy have pseudohypertrophy of their calves. Observation and functional analysis help assess coordination in infants and toddlers. Exchanging toys or objects with the child permits assessment of intention tremor and dysmetria (errors in judging distance), signs of cerebellar dysfunction. Cooperative children can do repetitive finger or foot tapping to test rapid alternating movements. Cerebellar and corticospinal tract dysfunction produce slowing and irregularity during tests of rapid alternating movements. The sensory examination of newborns and infants is limited to observing the behavioral response to light touch or gentle sterile pinprick. In a cooperative child, the senses of pain, touch, temperature, vibration, and joint position can be tested individually. The cortical areas of sensation must be intact to identify an object placed in the hand (stereognosis) or a number written in the hand (graphesthesia) or to distinguish between two sharp objects applied simultaneously and closely on the skin (two-point discrimination). Spikes, polyspikes, and spike-and-wave abnormalities, either in a localized region (focal) or distributed bihemispherically (generalized), indicate an underlying seizure tendency. Spontaneous discharge of motor fibers (fibrillations) or groups of muscle fibers (fasciculation) indicates denervation, revealing dysfunction of anterior horn cells or peripheral nerves. Abnormal muscle responses to repetitive nerve stimulation are seen with neuromuscular junction disorders, such as myasthenia gravis and botulism. The amplitude and duration of the muscle compound action potentials are decreased in primary diseases of muscle. Cranial ultrasonography is a noninvasive bedside procedure used to visualize the brain and ventricles of infants and young children with open fontanelles. There are three key features present: background patterns, behavioral state modulation, and presence or absence of epileptiform patterns. The background varies with age, but there should be general symmetry and synchrony between the background of the two hemispheres without any localized area of higher amplitude or slower frequencies (focal slowing). Fixed slow wave foci (1 to 3 Hz) delta rhythms suggest an underlying structural abnormality (brain tumor, abscess, stroke). Headaches can be a primary problem (migraines, tension-type headaches) or secondary to another condition. Secondary headaches are most often associated with minor illnesses such as viral upper respiratory infections or sinusitis, but may be the first symptom of serious conditions (meningitis, brain tumors), so a systematic approach is necessary. Each pattern (acute, recurrent-episodic, chronic-progressive, chronic-nonprogressive) has its own differential diagnosis (Table 180-1). Tension-type headaches are the most common recurrent pattern of primary headaches in children and adolescents. The pain is global and squeezing or pressing in character, but can last for hours or days. Headaches can be related to environmental stresses or symptomatic of underlying psychiatric illnesses, such as anxiety or depression. Migraine headaches are another common type of recurrent headaches and frequently begin in childhood. Headaches are stereotyped attacks of frontal, bitemporal, or unilateral, moderate to severe, pounding or throbbing pain that are aggravated by activity and last 1 to 72 hours. Associated symptoms include nausea, vomiting, pallor, photophobia, phonophobia, and an intense desire to seek a quiet dark room for rest. Toddlers may be unable to verbalize the source of their discomfort and exhibit episodes of irritability, sleepiness, pallor, and vomiting.
Syndromes
- Bladder stones
- Your child may breathe saliva and fluids from the stomach into the lungs. This is called aspiration. It can cause choking and pneumonia (lung infection).
- Watered-down fruit juice or broth may also help.
- Infection with the organism that causes babesiosis
- Pulse oximetry to measure blood oxygen level
- Birth control pills
- Infection such as pneumonia or sepsis
- Arthritis
Generic udenafil 100 mg
In cases of hemolytic anemia osbon erectile dysfunction pump udenafil 100 mg purchase overnight delivery, free hemoglobin not bound to haptoglobin appears in the urine erectile dysfunction see urologist udenafil 100 mg buy otc. Examination should include measurement of blood pressure erectile dysfunction therapy treatment generic udenafil 100 mg with visa, fluid balance erectile dysfunction doctors in ny cheap udenafil 100 mg buy online, and cardiac status, and an evaluation for signs of vasculitis or other systemic disease. A complete set of laboratory blood tests, including blood counts (with white cell differential) and biochemical studies for kidney function, electrolytes, albumin, globulins, cholesterol, calcium, phosphate, liver function tests, and uric acid should be sent. In addition, an immunology screen and virology testing in those patients deemed at risk is indicated. A kidney ultrasound is necessary to evaluate kidney sizes and structural abnormalities before a kidney biopsy is performed. The presence of proteinuria on a screening dipstick should be confirmed by laboratory analysis and quantification. The dipstick should be repeated on at least one other occasion, and if subsequent tests are negative, possible causes of false-positive results (such as radiocontrast agents) or transient proteinuria should be considered. Orthostatic proteinuria should be considered in adolescent patients (frequency of 2% to 5%), but it is uncommon in those older than 30 years. It is characterized by increased protein excretion in an upright position but normal protein excretion when supine. The exact pathophysiology is unclear, but total protein excretion rarely exceeds 1 g/24 h. The diagnosis can be confirmed with a split 24-hour urine collection with urine produced during the night and during the day collected in separate containers. Orthostatic proteinuria is a benign condition that requires no further follow-up and often abates with time. Kidney biopsy should be considered if: · P roteinuria is of glomerular or tubular origin without a clear cause. In patients with longstanding diabetes and progressive microalbuminuria, a kidney biopsy is not justified. However, it is more difficult to evaluate a diabetic patient who suddenly develops nephrotic range proteinuria, because a minority will have other glomerular pathologies. Similarly, hypertensive patients often have low-level proteinuria, but sudden onset nephrotic syndrome often has another cause. Immunologic testing identifies circulating autoantibodies, abnormal complement levels, and pathologic immunoglobulins or immune complexes. A positive rheumatoid factor in the setting of proteinuria is associated with cryoglobulinemia in a patient with proteinuria (see. In an older patient, occult malignancy may present as proteinuria associated with membranous nephropathy or membranoproliferative glomerulonephritis (commonly carcinoma of the breast, colon, stomach, and lung). Hodgkin and non-Hodgkin lymphomas are associated with minimal change nephropathy, and monoclonal gammopathies are associated with fibrillary glomerulopathy and overflow proteinuria. Myoglobinuria in the absence of muscle injury requires evaluation for drug toxicity or inherited muscle enzyme deficiency. Hemoglobinuria can be caused by intravascular hemolysis (such as paroxysmal nocturnal hemoglobinuria). Tubular proteinuria can be quantified and monitored by assessment of the ratio of the excretion rate of 2microglobulin to that of albumin. Factitious addition of egg albumin or other proteins to the urine can be detected by urine electrophoresis. Patients with tubular proteinuria should be screened for heavy metal (cadmium, lead, antimony) toxicity and also for systemic disease (Sjцgren syndrome, malignancy). Gaspari F, Perico N, Remuzzi G: Timed urine collections are not needed to measure urine protein excretion in clinical practice, Am J Kidney Dis 47:8-14, 2006. Part 2: Patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation and follow-up, Urology 57:604-610, 2001. National Kidney Foundation: Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation Classification and Stratification.
Purchase udenafil 100 mg with visa
Selective IgA deficiency is defined as serum IgA levels less than 10 mg/dL with normal levels of other immunoglobulins intracorporeal injections erectile dysfunction buy udenafil 100 mg amex. The diagnosis cannot be confirmed until the patient is at least 4 years of age when IgA levels should reach adult levels erectile dysfunction in young males causes 100 mg udenafil buy visa. In others it is associated with recurrent sinopulmonary infections xeloda impotence 100 mg udenafil order, IgG2 subclass deficiency erectile dysfunction drugs in nigeria udenafil 100 mg buy amex, specific antibody deficiency, food allergy, autoimmune disease, or celiac disease. IgG subclass deficiency occurs when the level of antibodies in one or more of the four IgG subclasses is selectively decreased while total IgG levels are normal. Normal individuals can express low levels of one or more subclasses, so a history of recurrent infections is important. An inability to synthesize specific antibody titers to protein or polysaccharide antigens is the best marker of IgG subclass deficiency associated with recurrent infections and requiring therapy. Transient hypogammaglobulinemia of infancy is a temporary condition characterized by delayed immunoglobulin production. The pathogenesis of this disorder is unknown but is thought to result from a prolongation of the physiologic hypogammaglobulinemia of infancy. The immunoglobulin nadir at 6 months of age is accentuated, with immunoglobulin levels less than 200 mg/dL. Immunoglobulin levels remain diminished throughout the first year of life and usually increase to normal, age-appropriate levels, generally by 2 to 4 years of age. The diagnosis is supported by normal levels of both B and T cells and by normal antibody responses to protein antigens such as diphtheria and tetanus toxoids. The transient nature of this disorder cannot be confirmed, however, until immunoglobulin levels return to normal ranges. Lack of specific antibody titers explains the recurrent infections and justifies therapy. Combined Immunodeficiency Diseases Decision-Making Algorithms Available @ StudentConsult. Hyper-IgM syndrome is characterized by a failure of immunoglobulin isotype switching from IgM and IgD to IgG, IgA, or IgE, and a lack of memory responses. Affected patients have normal or elevated serum levels of IgM with low or absent levels of IgG, IgA, and IgE. These forms of hyper-IgM are antibody deficiency diseases and not combined immunodeficiencies (see Table 73-1). Most patients exhibit severe infection early in life, although the diagnosis in patients with partial enzyme function may not be established until after 5 years of age or, occasionally, in adulthood. Patients with late-onset diagnosis are generally lymphopenic; they may have B cells and normal total immunoglobulin levels but little functional antibody (Nezelof syndrome). Most, but not all, patients with DiGeorge syndrome have a defect on chromosome 22q11. DiGeorge syndrome is classically characterized by hypocalcemic tetany, conotruncal and aortic arch anomalies, and increased infections. Most patients have partial immune defects with low T-cell numbers and function that generally improve with age. Wiskott-Aldrich syndrome is an X-linked disorder characterized by thrombocytopenia, eczema, defects in cell-mediated and humoral immunity, and a predisposition to lymphoproliferative disease (Table 73-3). Deficiency of this protein results in elevated levels of IgE and IgA, decreased IgM, poor responses to polysaccharide antigens, waning T-cell function, and profound thrombocytopenia. Opportunistic infections and autoimmune cytopenias become problematic in older children. Isolated X-linked thrombocytopenia also results from mutations of the identical gene. One third of patients with Wiskott-Aldrich syndrome die as a result of hemorrhage, and two thirds die as a result of recurrent infection caused by bacteria, cytomegalovirus, P. Stem cell transplantation has corrected the immunologic and hematologic problems in some patients. Patients with Omenn syndrome have T cells in the periphery, but these T cells have a limited repertoire. IgA deficiency, IgG2 subclass deficiency of variable severity, low IgE levels, and variably depressed T-cell function may be seen. There is normal antibody production but significantly decreased or absent lymphocyte proliferation and delayed skin reactivity to Candida.
Buy discount udenafil 100 mg on line
In the rat erectile dysfunction at 21 discount udenafil 100 mg mastercard, phosphate reabsorption is greatest in the duodenum and the jejunum erectile dysfunction doctor edmonton udenafil 100 mg buy, with very little occurring in the ileum erectile dysfunction causes prescription drugs udenafil 100 mg buy with mastercard. By contrast erectile dysfunction 27 order udenafil 100 mg on line, in the mouse, Pi is absorbed along the entire intestine with the highest levels of Pi reabsorption occurring in the ileum. The human pattern of intestinal phosphate reabsorption is thought to resemble that found in the rat. Renal Regulation of Phosphate Balance the kidney plays a key role in phosphate homeostasis. In normal adults, between 3700 and 6100 mg/d of phosphorus is filtered by the glomerulus (Figure 1B). Net renal excretion of phosphorus is between 600 and 1500 mg/d, which means that between 75% and 85% of the daily filtered load is reabsorbed by the renal tubules. Maintenance of normal serum phosphorus levels is primarily achieved through a tightly regulated process of Pi reabsorption from the glomerular filtrate. Within the nephron, approximately 85% of phosphate reabsorption occurs within the proximal tubule (Figure 3B). The remainder of the nephron plays a minor role in Pi regulation and the transporters involved have yet to be identified (22). Within the proximal tubule, Pi transport from the ultrafiltrate across the proximal tubule epithelium is an energydependent process that requires sodium (23). The three renal sodium phosphate cotransporters, Npt2a, Npt2c, and PiT-2, are all positioned in the apical brush border membrane of renal proximal tubule cells and use the energy derived from the transport of sodium down its gradient to move inorganic phosphate from the luminal filtrate into the cell (Figure 6). The amount of phosphate reabsorbed from the filtrate is determined by the abundance of the cotransporters in the apical membrane of proximal tubule cells and not by any alterations in the rate or affinity of Pi transport by posttranscriptional modifications (23). Thus, hormones or dietary factors that alter phosphate reabsorption in the kidney do so by changing the abundance of the sodium phosphate cotransporters in the apical membrane of renal proximal tubule cells. An increase in the brush border levels of the sodium phosphate cotransporters abundance results in increased phosphate absorption from the urine, whereas a decrease in cotransporter abundance leads to phosphaturia. Transport of Pi from the renal proximal tubule to the peritubular capillaries occurs via an unknown basolateral transporter (24). Within the proximal tubule in rats and mice, the abundance of Npt2a gradually decreases along the proximal tubule, whereas Npt2c and PiT-2 are expressed mainly in the first (S1) segment (29). Work from knockout studies in rodents has shown that in mice, Npt2a is responsible for the majority (approximately 70%) of the renal regulation of phosphate transport (29). By contrast, linkage analyses have found that in humans, Npt2a and Npt2c may contribute equally to phosphate reabsorption (30,31). The importance of PiT-2 in the renal control of Pi in humans remains unclear (20). There are a number of functional differences between the three cotransporters (Figure 6). However, Npt2a is electrogenic, transporting three sodium ions into the cell for every one phosphate ion, whereas Npt2c is electroneutral, transporting two sodium ions for every one phosphate ion (32,33). PiT-2, on the other hand, although electrogenic like NaPi2a, preferentially transports monovalent phosphate (23). Renal control of phosphate reabsorption is regulated by a number of hormonal and metabolic factors (Table 2) that are discussed below in more detail. These factors change 1264 Clinical Journal of the American Society of Nephrology Figure 6. Pi is reabsorbed via three sodium phosphate cotransporters: Npt2a, Npt2c and PiT-2. In humans, Npt2a and Npt2c are believed to play the most important role in phosphate reabsorption. The sodium phosphate cotransporters, which are positioned in the apical membrane of renal proximal tubule cells, use energy derived from the movement of sodium down its gradient to move Pi from the filtrate to the cell interior. The amount of phosphate reabsorbed is dependent on the abundance of the sodium phosphate cotransporters in the apical brush border membrane and hormones such as parathyroid hormone and fibroblast growth factor-23 decrease Pi reabsorption by decreasing the abundance of the sodium phosphate cotransporters in the brush border. Movement of phosphate from the interior of renal proximal tubular cells to the peritubular capillaries occurs via an unknown transporter.
Discount udenafil 100 mg fast delivery
In an acute infection erectile dysfunction treatment heart disease discount 100 mg udenafil overnight delivery, heterophile antibodies usually appear on Monospot within the first 3 weeks of illness erectile dysfunction in diabetes treatment cheap udenafil 100 mg free shipping, but then decline rapidly within a few weeks erectile dysfunction treatment otc cheap udenafil 100 mg buy on-line. These patients may have serologic negative tests because of their immunosuppression impotence drugs 100 mg udenafil purchase with visa. This test is performed to detect hereditary spherocytosis and thalassemia when intravascular hemolysis is identified. This produces membrane instability, which forces the cell to the smallest volume-that of a sphere. A single-tube osmotic fragility test has been proposed for thalassemia screening with a range of different saline concentrations. E Interfering factors · Acute hemolysis the osmotically labile cells are already hemolyzed and, therefore, not found in the blood specimen. Testing is 392 erythrocyte fragility recommended during a state of prolonged homeostasis with stable hematocrit. It is nonspecific and therefore not diagnostic for any particular organ disease or injury. Other physicians regard this test as so nonspecific that it is useless as a routine study. Interfering factors · Artificially low results can occur when the collected specimen is allowed to stand longer than 3 hours before the testing. Abnormal findings Increased levels Chronic renal failure Malignant diseases Bacterial infection Inflammatory diseases Necrotic tissue diseases Hyperfibrinogenemia Macroglobulinemia Severe anemias. This feedback mechanism is very sensitive to minimal persistent changes in oxygen levels. Occasionally athletes, in order to improve oxygen-carrying capacity and thereby improve performance, abuse this hormone. In contrast, diffuse esophageal spasm is characterized by strong, frequent, asynchronous, and nonpropulsive waves. Acid reflux with pH probe Acid reflux is the primary component of gastroesophageal reflux. If they coincide with patient symptoms of chest pain, esophagitis can be incriminated. Trans-nasal pH catheters can cause discomfort in patients, sometimes resulting in the avoidance of pH testing. With the wireless pH probes, patients can eat and drink normally as well as engage in their usual activities while having their pH levels tested. It collects pH data in the esophagus and transmits them via radio frequency telemetry to an external, pager-sized receiver worn by the patient. This allows patients to maintain regular diet and activities during the monitoring period (24 to 48 hours). This small pH capsule is attached to the wall of the esophagus by esophagoscopy (p. After the study is completed, the patient returns the receiver, and the data are downloaded to a computer for analysis. Acid clearing Patients with normal esophageal function can completely clear hydrochloric acid from the esophagus in less than 10 swallows. Patients with decreased esophageal motility (frequently caused by severe esophagitis) require a greater number of swallows to clear the acid. Bernstein test (acid perfusion) the Bernstein test is simply an attempt to reproduce the symptoms of gastroesophageal reflux. Contraindications · Patients who cannot cooperate · Patients who are medically unstable Potential complications · Aspiration of gastric contents esophageal function studies 399 Interfering factors · Eating shortly before the test may affect results. Instruct the patient not to eat or drink anything for at least 8 hours before the test. The tubes are equipped so that pressure measurements can be taken at 5-cm intervals (Figure 20).
Buy udenafil 100 mg online
For breast cancer erectile dysfunction over the counter 100 mg udenafil buy with amex, subgroup analyses in four cohort studies consistently found that calcium intake in the range of 780 to 1750 mg/d in premenopausal women was associated with a decreased risk for breast cancer erectile dysfunction medication canada 100 mg udenafil buy amex. For prostate cancer erectile dysfunction mayo clinic purchase 100 mg udenafil amex, three of four cohort studies found significant associations between higher calcium intake (>1500 or >2000 mg/day) and increased risk of prostate cancer erectile dysfunction bp meds cheap udenafil 100 mg free shipping, compared to men consuming lower amount of calcium (500-1000 mg/day). To address this issue in May and September of 2007, two conferences were held on the topic of vitamin D and health. Sources, Metabolism and Functions of Vitamin D Vitamin D was classified as a vitamin in the early 20th century and in the second half of the 20th century as a prohormone ("conditional" vitamin). The chemical difference between vitamin D2 and D3 is in the side chain; in contrast to vitamin D3, vitamin D2 has a double bond between carbons 22 and 23 and a methyl group on carbon 24. The efficiency of the conversion of 7-dehydrocholesterol to vitamin D3 is dependent on time of day, season of the year, latitude, skin color and age. The major naturally occurring food sources include fatty fish, beef liver and egg yolk. Dietary vitamin D is absorbed from the intestine and circulates in plasma bound to a vitamin D binding protein. Major sites of action include intestine, bone, parathyroid, liver and pancreatic beta cells. Biological actions include increases in intestinal calcium absorption, transcellular calcium flux and opening gated calcium channels allowing calcium uptake into cells such as osteoblasts and skeletal muscle. One of the major biological functions of vitamin D is to maintain calcium homeostasis which impacts on cellular metabolic processes and neuromuscular functions. Vitamin D affects intestinal calcium absorption by increasing the expression of the epithelial calcium channel protein, which in turn enhances the transport of calcium through the cytosol and across the basolateral membrane of the enterocyte. Additional sources include commercial white bread made with calcium sulfate, foods made with milk products, leafy greens, canned fish and calcium fortified foods. This process occurs primarily in the duodenum and proximal jejunum, is saturable, is energy dependent, and involves a calcium binding protein. This process is passive (does not depend on carrier proteins or energy) and occurs primarily in the jejunum and ileum. Calcium is absorbed between cells, rather than through cells, and down the concentration gradient. Calcium can be transported in blood bound to albumin and prealbumin, complexed with sulfate, phosphate or citrate, or in a free (ionized) state. Calcium is transported in blood bound to proteins (~40 percent), primarily albumin and prealbumin, complexed with sulfate, phosphate or citrate (~10 percent), and in the ionized form (~50 percent). Blood calcium concentrations are controlled extracellularly by parathyroid hormone, calcitriol and calcitonin. Increased intracellular calcium concentrations occur in response to second messengers by stimulating release from intracellular sites (endoplasmic reticulum, mitochondria) and hormones by facilitating influx from extracellular sites by transmembrane diffusion or channels. Calcium balance measures provide information on calcium absorption relative to calcium loss in urine, sweat and endogenous intestinal secretions. During periods of growth, positive calcium balance implies bone mineralization but does not provide an indication of whether the rate of bone mineralization is optimal. During adulthood negative calcium balance implies calcium lost from bone but does not provide an indication of which site(s). Calcium balances measures provide an indication of current but not prior calcium balance. An alternate approach to assessing bone mineralization is by measuring bone mineral density. These functions of calcium are frequently classified into the following general categories; bone development and maintenance, blood clotting, transmission of nerve impulses to target cells, muscle contraction and cell metabolism. In addition, calcium may play a role in colon cancer, kidney stones, blood pressure, body weight and lead absorption. Experience has shown that in the absence of unlimited resources, only a limited set of 20 questions can be addressed. Age specific intermediate or surrogate outcomes will need to be identified by the committee when few or no studies directly link specific nutrient intakes with clinical outcomes. Preferably, these would include only validated surrogates of the clinical outcome, that is outcomes that are strongly correlated with the clinical outcome. When a nonvalidated intermediate outcome must be considered, the implicit assumption is that they would have the properties of a validated surrogate outcome. Not only should this assumption be made explicit, but the uncertainties involved in applying this assumption should be identified, documented, and discussed by the committee.