
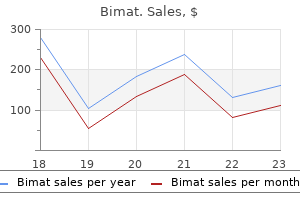
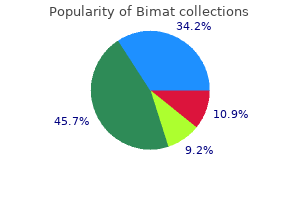
Bimat
John Tidy MD FRCOG
- Consultant Gynaecological Oncologist, The Jessop Wing,
- Sheffield
Private landlords have greater flexibility than state or federally subsidized programs in the selection of tenants symptoms genital herpes bimat 3 ml order on-line, but they are subject to Fair Housing Laws treatment vitiligo order bimat 3 ml online, which prohibit discrimination on the basis of: sex; race; age; disability; color medicine 44-527 buy generic bimat 3 ml on-line, creed or national origin; religion or familiar status symptoms quitting weed bimat 3 ml purchase without prescription. However, as a practical matter in the private rental market, income based barriers are the primary reason for exclusion. The two federal tenant based rental assistance programs are the Certificate Program and the Housing Voucher Program. The primary difference between the two programs is that there is no cap on rent level in the Voucher Program. If the tenant is willing to pay more than the allocated rental subsidy, they may do so. In most rental certificate programs, a family pays either 30% of its monthly adjusted gross income, 10% of its monthly gross income, or the welfare assistance designated for housing toward rent, whichever is greater. However, this does not affect the amount of rent a landlord may charge or the family may pay. A family or individual is free to choose any housing that meets the requirements of the program where the owner agrees to rent under the program. The goal of the program is to enable these households to move from homelessness or temporary emergency housing into more permanent housing and to return to self-sufficiency. The first significant federal legislation aimed at addressing homelessness was the McKinney Homeless Assistance Act of 1987. Transitional housing: Supportive housing that is designed to move homeless people into permanent housing. Safe havens: A structure or clearly identifiable portion of a structure that serves hard to reach homeless people with serious mental illnesses. Building specific housing: this program involves units located in identified buildings that are owned by private landlords, nonprofit organizations, or public entities, and often involves purchasing and developing the building or partnering with a private housing developer. The public mental health commission selects a building or development and helps the consumer rent there. The building specific model can be either mixed population or single purpose housing. Tenants represent several groups in mixed population housing, including people with mental illness, the elderly, low income and moderateincome individuals and families. In single purpose housing, people with mental illness occupy all units, and the building is not integrated. Episode of homelessness: A separate, distinct, and sustained stay on the streets and/or in an emergency shelter and the person must be unaccompanied and disabled during each episode. A Housing Toolkit: Information to help the public mental health community meet the housing needs of people with mental illness. To qualify, the person can have no other residence; and must lack the resources or support networks. Housing First: A program that features quick access to permanent housing for people who are homeless. Support services are available following the placement in order to provide housing stability and meet individual needs. However, housing is contingent only upon meeting the terms of a lease rather than with treatment compliance. These programs often require individuals to progress through several types of housing placements before receiving access to permanent housing. Low Demand Housing: Low-Demand Housing allows people in need of support services to determine the type and intensity of services they receive instead of requiring them to comply with pre-existing service plans. In the supportive housing model, services are available to the tenant, but accepting services cannot be required or in any way impact the tenancy. The supportive services may be provided by the organization managing the housing or coordinated by the applicant and provided by other public or private service agencies. Permanent housing can be provided in one structure, in several structures at one site, or in multiple structures at scattered sites. Housing Act of 1937 or under any state or local program that has the same general purposes as the federal program. This type of housing is limited to individuals and families whose income is below 80 percent of the median income in the county or metropolitan area in which they live.
As well treatment thesaurus trusted bimat 3 ml, convictions for non-contact sex offences have been consistently related to increased sexual recidivism risk (Helmus & Thornton medicine abuse generic 3 ml bimat, 2015) medicine bow 3 ml bimat purchase otc. Information Required to Score this Item: To score this item you must have access to an official criminal record as compiled by police or other law enforcement agencies medicine dictionary prescription drugs bimat 3 ml order on line, court, or correctional authorities. Self-report of criminal convictions may not be used to score this item except in specific rare situations, please see sub-section "Self-report and Static-99R", pages 8 to 9 in the Introduction section. To count an offence in this item, it must meet the general definition of a sex offence (see pages 20 to 28) in addition to meeting the definition of a non-contact offence (see below). Note that if the offender has a Category "A" offence somewhere on their record, then Category "B" offences can be counted for this item (including offences without a sexual motive, such as public urination). Anything that counts as a conviction or sentencing date would count for this item, if the behaviour was for a non-contact sex offence. The general definition of a non-contact sex offence is the following: Any illegal sexual act where the offender did not physically touch the victim or any physical touching that occurred was incidental to the offending, and either of the following: 1) the victim is actively coerced into nothing beyond perceiving. This latter category includes actions such as possession of child pornography and most voyeuristic behaviours including both live "peeping" and/or surreptitiously recording individuals in settings where privacy would normally be expected. By this rule, compelling the commission of a sex offence counts as a contact offence, even if there is no physical contact between the offender and the victim. Similarly, restraining and forcing a boyfriend to watch his girlfriend being sexually assaulted represents a contact sex offence because the boyfriend is being physically restrained or positioned in some way. Sending the boyfriend a videotape of his girlfriend being sexually assaulted represents a non-contact sex offence. Blackmailing a teenager to undress or masturbate represents a contact offence, whether or not the offender was present at the time, because the victim is coerced into participating in a sexual activity (not just perceiving it) and the offender deliberately made the victim aware of the victimization. Note that the current definition is not identical to the definition described in the previous Harris et al. The reason for the change is to address inconsistencies in the previous scoring rules, particularly relevant to internet offences, which were rare when the original coding rules were developed. These types of offences require a more nuanced scoring rather than considering all internet sex offenders as one homogenous group. The results will generally mean lower scores for some internet offenders, which is consistent with their generally lower risk. This new definition also allows greater consistency and flexibility when applied to novel offences. In cases where it is a judgement call the evaluator should consider that non-contact offences are often repetitive and more reflective of paraphilic interests and not reflective of behaviours designed to result in normative sexual contact. For example, an offender convicted of "trespassing" for peeping would get the risk point. When the offence details are unknown, it is possible to score this item based on the names of the offences. When the offence details are unknown and the offence name does not exclusively restrict its scope to non- contact sex offences, the offender would receive a score of "1" if the offence name is usually used for non-contact sex offences. In the case of "Criminal Trespass" or "Trespass by Night," the offence may be related to either voyeurism or break and enter. For example, if the offender has numerous break and enter convictions (which were not sexually motivated) and denies a sexual motivation in the trespassing, you would likely not count it on the grounds that a non-sexual motive is highly plausible. However, if the offender has a lengthy sexual offending record or has a history of or interest in voyeurism, the trespass can be presumed sexual based on a Balance of Probabilities. Institutional rule violations, charges, and arrests do not count, nor do self-reported offences. The index offence(s) may include a conviction for a non-contact sex offence and this conviction can count as a non-contact sex offence. If the offender is convicted in the same sentencing occasion of a contact sex offence such as lewd and lascivious behaviour with a child and a non-contact sex offence such as using an underage person for obscene matters, then the item is scored 1 since the offender committed a non-contact offence. The offender is subsequently 72 convicted of Sexual Interference (the Canadian term for a sex offence involving a victim under 16 years old) and Possession of Child Pornography. Attempted contact offences Sex offences in which the offender intended to make contact with the victim (but did not succeed) would be considered attempted contact offences and are coded as contact offences because of their intention. Internet crimes None of the Static-99R samples had enough internet-only offenders to provide for meaningful analysis. As a result, determining how to score internet crimes on Static-99R requires interpretation beyond the available data. Internet crimes can be roughly divided into two distinct groups because they seem to include elements of either contact or non-contact offences.
These treatments may be helpful symptoms 0f parkinson disease bimat 3 ml buy overnight delivery, but would not be currently recommended as a first-line treatment 3 medications that cannot be crushed discount 3 ml bimat visa. Occasionally a treatment may be included that medicine for nausea 3 ml bimat mastercard, though sometimes used in clinical practice medications vertigo 3 ml bimat buy, has not been tested. Treatment meets the criteria for none of the above categories because it is untested. The benefits and risks are unknown and caution (for providers or administrators) is suggested in applying them and or (for families) in receiving such treatment. What Seems to Work What Does Not Work Not Adequately Tested Untested Source: Virginia Commission on Youth Graphic, 2010. Accordingly, data should be collected to justify treatment plans, changes in treatment plans, and terminations. Clinicians and mental health treatment organizations are becoming both data-driven and data collectors, allowing for greater opportunities for outcome measures to be collected and reviewed over time. Revisions Made in Collection 5th Edition the Collection provides information that represents the medical model, the traditional approach to the diagnosis and treatment of medical conditions. This model focuses on the physical and biological aspects of specific diseases and conditions. However, the medical model does not incorporate changes in the language or methods used for communicating and interacting with individuals with developmental disabilities. In interacting with youth with developmental disabilities, a service provider can use "person-centered" planning and approaches to focus on emotional and support needs. Person-centered practices promote individualized treatment and service plans, in addition to emphasizing individualized outcomes and the participation of the individual in their treatment planning. Further, these plans focus on the services needed for the youth to address his or her mental health disorder and to lead successful integrated lives in their community (National Association of State Mental Health Program Directors, 2004). In response to the above-referenced finding, the Commission on Youth adopted the following recommendations at its November 2011 meeting: 1. The Commission on Youth will revise the Autism Spectrum Disorders and Intellectual Disability sections of the Collection 4th Edition and limit these sections to discussion of cooccurring mental health disorders. The Commission on Youth will add a disclaimer to the Collection 5th Edition to acknowledge that Intellectual Disability and Autism Spectrum Disorders are developmental disorders. The Commission on Youth will convene the Advisory Group prior to the 2013 biennial update and discuss further modifying the Intellectual Disability and Autism Spectrum Disorders sections to include best practices in service delivery for developmental disabilities. Accordingly, information included in the "Developmental Disabilities" section of the Collection 5th Edition is provided in response to these recommendations. Conclusion Effective mental health treatments which have undergone testing in both controlled research trials and real-world settings are available for a wide range of diagnosed mental health disorders. The Collection 5th Edition is designed to encourage use of these treatments by professionals providing mental health treatments. The Collection 5th Edition is also designed to inform parents, caregivers, and other stakeholders by providing general information about the various disorders and problems affecting children and adolescents. Evidence-based treatments have been developed with the express purpose of improving the treatment of child and adolescent mental health disorders (Nock et al. Clinicians can incorporate these well-documented treatments, while still adequately addressing the individual differences of the patient (Nock et al. Prevalence of Autism Spectrum Disorders - Autism and Developmental Disabilities Monitoring Network, 14 Sites, United States, 2008. The prevalence of serious emotional disturbance: a re-analysis of community studies. From science to practice: the flexible use of evidence-based treatments in clinical settings. Journal of the American Academy of Child and Adolescent Psychiatry, 43 (6), 777-780. National estimates of mental health utilization and expenditures for children in 1998, in Blueprint for Change: Research on Child and Adolescent Mental Health, Vol. National estimates of mental health utilization and expenditures for children in 1998. Mental Health: Culture, Race, Ethnicity Supplement to Mental Health: Report of the Surgeon General. The role of education in a system of care: effectively serving children with emotional or behavioral disorders. Families are coming to understand that evidence-based practices are those which have been shown through research to be effective.
An emergency facility or an agent or employee of an emergency facility acting in compliance with the Emergency Evaluation statute is exempt from civil or criminal liability symptoms mercury poisoning order bimat 3 ml on-line. The Department is subrogated against any insurance coverage available to the patient for charges related to emergency service symptoms of kidney stones cheap bimat 3 ml online, initial consultant examination symptoms kennel cough 3 ml bimat buy with amex, and transportation to an emergency facility treatment 5cm ovarian cyst buy discount bimat 3 ml on line. If the juvenile is less than 18 years of age, a parent or guardian is authorized by law to sign for admission. The Juvenile Court also has access to services in the event some less restrictive alternative is available. The form is readily available through courts, hospitals, police, mental health providers, and the internet. All other petitioners must appear before the judge and present the Petition for Emergency Psychiatric Evaluation. If the judge finds probable cause to believe that the evaluee has a mental disorder and poses a danger to the life of safety of himself or others, the judge endorses the petition. The judge should explain to the petitioner that the endorsement only authorizes examination of the evaluee and that the decision about hospitalization is up to the examining physician. It is also good practice for the judge to encourage the petitioner to coordinate with the officer who will be executing the petition and, if possible, to respond to the emergency facility to provide any needed information to the examiner. It is also important for the petitioner to speak with the police officer about the execution of the petition and whether the officer should expect a struggle or weapons. It is advisable for the petitioner to go to the emergency admitting facility when the evaluee is transported, so any background information needed by the examining physician can be provided. Upon transfer of custody of the evaluee to the emergency facility medical staff, the officer is generally not required to remain. The evaluee may not be detained for more than 30 hours, and must be discharged unless he or she agrees in writing to a voluntary admission or is certified by two physicians or one physician and one licensed psychologist as meeting the requirements for involuntary commitment. If the evaluee meets the standards for involuntary admission, the examining physician shall take the necessary steps for admission to an appropriate facility, which may be a general hospital with a licensed psychiatric unit. In the event the examining physician is unable to carry out the admission, the physician shall notify the Department. Within six hours, the Department shall provide admission to an appropriate facility. Mental Health Procedures (2014) Chapter 7 Emergency Psychiatric Evaluation 301 Section 7. Police dislike the statute because the process is labor intensive and time consuming. The officer must both transport the evaluee/arrested individual and remain with the evaluee during the examination. Unless the evaluee is admitted, the officer must return the evaluee to court or jail. The examining physician is required to prepare a brief report of the findings, which the officer must give to the court. If court is not in session when the evaluation is concluded, the officer must bring the evaluee and the report to court the next business day. If competency is an issue, many people find that the competency evaluation is the preferable route to take. The mentally ill arrestee who is at risk in the jail is placed in a hospital setting, and the competency evaluation moves the case forward. However, there may be occasions when this statute would be useful, such as when an arrestee has a mental disorder and presents a danger, but is competent to stand trial. It should also be noted that some local detention centers use the certification process for mentally ill detainees who meet the criteria for involuntary admission. A problem with this approach is that the detainee is in custody by court order, and the court is not involved with the involuntary admission by certificates. Mental Health Procedures (2014) Chapter 7 Emergency Psychiatric Evaluation 304 this page intentionally left blank for two-sided printing purposes. Mental Health Procedures (2014) Chapter 7 Emergency Psychiatric Evaluation 305 Section 7.
Depression has been consistently identified as the most common psychological disorder among adolescents who have committed suicide (Gould et al symptoms 8 dpo cheap bimat 3 ml with amex. Additionally medications 5 rs order bimat 3 ml with visa, there is a high prevalence of substance abuse among older adolescents symptoms high blood pressure bimat 3 ml sale, particularly males acute treatment 3 ml bimat buy otc, who commit suicide (Gould et al. There is also a particularly high prevalence of co-occurring depressive disorders and substance abuse among those who commit suicide (Gould et al. Youth most at risk of attempting suicide are likely to have recently experienced stressful life events, such as school and work problems, legal problems and interpersonal conflict (Gould et al. The research cited suggests that parental divorce and strained parent-child relationships may be factors, after accounting for parent and youth psychopathology (Gould et al. Other Risk Factors There are a number of environmental factors and distressing experiences associated with increased risk of suicide. McKeown, Cuffe and Schultz (2006) found that the presence of firearms in the home is significantly associated with higher rates of suicide. There is strong research evidence to suggest that abuse, both physical and sexual, is associated with increased risk of youth suicide (Gould et al. There is growing, though inconclusive, evidence for a contagion effect for youth suicide (Gould et al. Some studies have found that the suicide rate among adolescents rises following a highly publicized suicide. Family environment and genetic factors are associated with increased risk for suicide among youth. Additionally, family history of suicide and suicide attempts and parental psychopathology are associated with increased risk for youth suicide (Gould et al. Even after accounting for the effects of parental psychopathology, completed suicide by the mother corresponded with a fivefold increase in suicide by offspring, while completed suicide by the father corresponded with a doubling suicide by offspring (Gould et al. While suicide ideation is an important indication of risk for suicide (90 percent of youth who attempted suicide had previously reported suicide ideation), not every youth who reports thinking about death, hurting themselves or ending their lives will attempt suicide (Spirto & Overholser, 2003). The severity of hopelessness, isolation, suicidal ideation, and hesitation to discuss their suicidal thoughts are factors that may differentiate between youth who only contemplate death and suicide and those who, in fact, attempt to kill themselves. These are minimal standards which, by definition, are expected to apply in almost all cases and instances where these standards are not followed should be supported in the medical record. In addition, there are a number of standardized suicide measures that range from long and comprehensive to short screeners. If there is a recent history of suicidal ideation or suicidal behavior, the youth should continue to be monitored. Aids clinicians in determining the imminent danger of suicide A semi-structured diagnostic clinical interview designed for use with youth that provides a systematic approach for evaluating suicidality A structured diagnostic clinical interview that can be used to evaluate suicidality Variable 20-30 minutes 2. This questionnaire assesses the following: direct risk factors, including exposure to suicidal behavior, attitudes/beliefs about suicide, suicide ideation, suicide plans, and past suicide attempts; related risk factors, such as anger, anxiety, depression, and hopelessness; and protective factors, including support, self-esteem, coping, and personal control. The Imminent Danger Assessment provides the clinician with the following information about the youth: degree of hopelessness; ability to identify their emotions so that they can seek support prior to becoming suicidal; reason for saying that they are not suicidal (is the adolescent truly no longer suicidal or are they saying that they are no longer suicidal to avoid further discussion about the state of mind or to avoid hospitalization); ability to identify their support system; and ability to cope with suicidal tendencies (Goldston & Compton, 2007). Promising Practices in Youth Suicide Prevention Currently there are no treatments which have been deemed evidence-based; accordingly there is no table summarizing evidence-based treatments provided. Despite limited literature, however, there is research to support the use of some techniques over others. The following paragraphs summarize the literature regarding treatment focus, crisis management, and on-going treatment. In a review of the literature on treatments for suicide ideation, suicide attempts, and non-suicidal self-injurious behavior in both youth and adults, treatments which target suicidal behavior directly are shown to be effective (Miller, Rathus & Linehan, 2007). There is little research to support the effectiveness (as measured by number of suicide attempts or lethality of attempts) of treatments focusing on depression, bipolar disorder, and other underlying disorders associated with suicide (Miller, Rathus & Linehan). Spirito and Overholser note that, while it is important to treat the underlying psychopathology, such treatments do not necessarily reduce suicidal behavior (2003). In a related finding, a study looking at the outcome of two types of treatment for suicidal females, the 206 treatment that focused directly on suicidal behaviorDialectical Behavior Therapyoutperformed the treatment for the control groupcommunity treatment by an expert therapistin reducing suicide attempts. The treatments, however, did not differ in their effect on depressive symptoms (Linehan et al. Additionally, parents need to be directed to increase the level of supervision provided the youth. Department of Health and Human Services (2001) has outlined pharmacological interventions thought to be effective in reducing suicide.
Order 3 ml bimat overnight delivery. न्यूमोनिया का चमत्कारी घरेलू उपचार। Pneumonia treatment in ayurveda.
References
- Amelar RD, Hotchkiss RS: The split ejaculate: its use in the management of male infertility, Fertil Steril 16:46n60, 1965.
- Hu X, Bao Y, Zhang L, et al. Omitting elective nodal irradiation and irradiating postinduction versus preinduction chemotherapy tumor extent for limited-stage small cell lung cancer: interim analysis of a prospective randomized noninferiority trial. Cancer 2012;118(1):278-287.
- Deutschman CS, Wilton P, Sinow J, et al: Paranasal sinusitis associated with nasotracheal intubation: a frequently unrecognized and treatable source of sepsis. Crit Care Med 14:111, 1986.
- Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987;235:177-182.
- Montironi R: Intratubular germ cell neoplasia of the testis: testicular intraepithelial neoplasia, Eur Urol 41:651n654, 2002.
- Sigel JE, Smith TA, Reith JD, Goldblum JR. Immunohistochemical analysis of anaplastic lymphoma kinase expression in deep soft tissue calcifying fibrous pseudotumor: evidence of a late sclerosing stage of inflammatory myofibroblastic tumor? Ann Diagn Pathol 2001;5(1):10-4.